

The impacts of abuse and neglect on children; and comparison of different placement options: Evidence Review (open access)
Commissioned by the Department for Education and developed by Research in Practice, this open access paper reviews research on the impacts of abuse and neglect and the strengths and weaknesses of care placement options. It is intended to support local authority and judicial decision-makers to develop a shared understanding of research and make decisions that lead to stable and positive placements for children and young people.
1. Introduction and methodology
1.1 Introduction and aims of the review
Background
In recent years the government has introduced a number of policy papers aimed at transforming the children's social care system. 1 Much of this reform began in 2000 with the publication of Adoption: A new approach. 2 More recently, major changes have been introduced through the Family Justice Review 3; the subsequent Children and Families Act 2014 4, including the revised Public Law Outline (PLO) and the 26-week timeframe for completing care proceedings; and the recent publication of Putting Children First. 5
When the Family Justice Review was launched in 2011, the average duration for the disposal of a care and supervision application was 56 weeks. The revised PLO was phased in between July and October 2013 following a year-long pilot in the tri-borough authorities in London. Since then there has been a significant reduction in the duration of care proceedings with the average (at the time of writing) being around 27 weeks. 6 There is some recent evidence to suggest that this has been achieved without delay being moved to the pre- or post-court period 7, although this finding needs to be considered in the context of how cases are being managed by local authorities before formal proceedings are issued or during the pre-proceedings stage of the PLO.
The judiciary have acted as a strong driver for the completion of cases within the 26- week timeframe. However, beneath the national average statistics, proceedings duration for individual local authorities and for local family justice board areas vary significantly. 8 These reductions in care proceedings duration have taken place in the context of increasing demand on the public family law system and changes in the use of some types of order:
- The number of care applications continues to rise. Between April 2015 and March 2016, total applications were 15 per cent higher when compared to the same period in 2014-15. And in the first six months of 2016-17, the number of care applications increased by 23 per cent over the same period in the previous year, although there was a drop in December 2016. 9
- At 31 March 2016, there were 70,440 looked after children in England, an increase of one per cent compared to 31 March 2015, and an increase of five per cent compared to 2012. 10
- The use of special guardianship orders (SGOs) rose from five per cent of all children ceasing to be looked after in 2010, to 12 per cent in 2015-16. 11
- Since September 2013, the number of court confirmed plans for adoption has almost halved. From 2012, adoption levels were rising and reached a peak in 2013 -14 (9,080 children placed for adoption). From September 2013 this trend reversed, a change attributed by many to the impact of Re B-S and other court judgements. 12 The number of looked after children placed for adoption fell to 7,740 in 2015-16. 13
Aims
The initial impetus for the commissioning of this evidence review was a commitment set out in Adoption: A vision for change (2016) to produce 'an independent summary of relevant research evidence for use by local authority managers, social workers and judges which focuses on comparative outcomes of different placement options'. The government made this commitment in response to several factors, including the increase in the number of children entering the care system, shifts in patterns of decision making and the ongoing aim to ensure that factors known to be crucial to children's outcomes are considered when placement decisions are made. 14
The aim of this review is to bring together a summary of key research findings in one document intended to be accessible to judicial and local authority decision makers (although this will also be of interest to others including Cafcass guardians) with regard to two key themes:
- The impacts of abuse and neglect on children
- The strengths and weaknesses of different types of long-term placements in relation to their impact on children.
The review is intended to help decision makers (including Cafcass guardians) reflect on the needs of children who have been abused or neglected and understand how different placement types may address particular needs. We hope that the work undertaken here (between October 2016 and January 2017) provides a useful summary document that will support the complex series of decisions that lead to placements that are stable and positive for the children and young people concerned. Nevertheless, it is important to manage expectations from the start. This review does not offer definitive answers on the themes noted above.
Firstly, it is important to note that research has its limitations and bodies of evidence change over time. (The limitations of this review are considered at 1.3 below.) Decision makers need access to information that is comprehensive and regularly updated; this review offers a picture at the current time. Secondly, the application of research evidence in making decisions in relation to individual cases requires learning and development support and relies on those informing the decision making to have an in-depth understanding of the individual child, their family and wider context. There are no generic answers that research can provide that can be applied in a wholesale way across the specific case circumstances of individual children, young people and families. We can learn a great deal from the aggregated evidence that research provides, but that evidence only gains meaning when it is applied, with analytical rigour and critical thinking, to each individual situation. Thirdly, whilst this review is intended to be useful to decision makers in local authorities and within the judiciary, it is recognised that colleagues working in different parts of the system will have their own professional perspectives and areas of specialist expertise. This piece of work is therefore necessarily generic in the whole, and seeks to augment the existing more specialised knowledge sources.
1.2 Methodology and scope of the review
This paper is not a systematic review. A full systematic review of the extensive and various bodies of research in relation to the themes outlined above is beyond the scope of this commission. Rather, the aim is to provide a broad and accessible overview of the most relevant research. The primary focus of the review is on key UK research from 2000 to 2016. Reference is also made to key international evidence that has particular relevance to the review.
Evidence was drawn from peer-reviewed papers that either report on, or provide a robust review of primary research in relation to the key themes, along with a small number of policy papers and independent reviews. Searches were conducted using online databases (e.g. Social Care Online; Google Scholar) and broad search terms linked to the topic areas and themes of the review (e.g. impacts of abuse and neglect; educational outcomes for looked after children; placement stability). Given the timescales of the project, the initial focus was on searching for existing research reviews in relation to the key themes, with key research studies that were identified in the literature being explored in further detail. Searches were also made of key websites and repositories of relevant research and statistics. Guidance was sought on the scope and content of the review from an expert advisory group (see Appendix 1) set up by the Department for Education. Experts on the key themes of the review were also consulted to critically appraise the content of the report.
A key challenge for this evidence review was the need to strike a balance between rigour and accessibility, without over-simplifying the evidence. Of particular importance was the need for clarity with regard to the robustness of the research and caution in attributing causality when presenting the findings. To address this, an appendix has been included which summarises the methodological approaches used in key research papers that are referred to in this report and any limitations to the findings. Given the critical importance of the decision making this review is intended to support, readers are strongly encouraged to read this appendix.
1.3 Limitations and considerations
When considering the evidence in this review it is important to bear in a mind a number of considerations.
- Research findings do not tend to identify outcomes for individual children. Children and young people who are the subject of care proceedings are all individuals with specific social, cultural, familial and genetic characteristics. All of them develop their identity within some form of family relationships and all have specific experiences and vulnerabilities. This myriad of factors can result in children and young people having differing susceptibilities and resiliencies in the face of adverse experience, so the outcomes for one child may be very different to those of another, even within the same family. 15 So, while findings from research relating to specific groups or specific outcomes are helpful in informing decisions, they cannot predict outcomes for individual children.
- There is not an equal body of literature, in scale or rigour, available in relation to each of the issues raised in this report. Some topics have benefited from high quality research whilst others are less represented in the literature. This presents challenges in offering direct comparisons between impacts of different types of harm or between types of placement.
- As with much social research, it is often extremely difficult to determine the direction of cause-effect relationships. The 'gold standard' for research in determining whether a cause-effect relationship exists is the use of a randomised controlled trial (RCT), where individuals are randomly allocated to a 'treatment' or 'control' group. RCTs minimise bias and control for extraneous factors. RCTs are rarely used in research pertaining to children's social care in England 16, partly because of the ethical issues that are raised by the random allocation of children to different placement options or therapeutic interventions or to control groups.
- As a result, other robust research designs are used. These generally include the use of comparison measures between or within groups (e.g. comparing mental health outcomes for looked after and non-looked after children) and explore statistical associations between factors thought to be linked to particular outcomes. In addition, qualitative studies are used to answer different kinds of research questions and to provide more in-depth and explanatory information (e.g. to explore the values and contextual issues that inform professional decision making or the perceptions of service users and professionals).
- Research evidence evolves over time and interacts with current policy priorities and with public consciousness and as such, does not provide fixed solutions or definitive answers for decision making at individual case level. The application of research evidence in practice requires nuanced professional judgement and sophisticated analytical skills from senior decision makers in local authorities as well as the judiciary.
- Some of the research (e.g. the evidence on neurobiology and brain functioning) is relatively recent, and the evidence base is still developing and subject to some debate. Interpreting this research for application in policy or individual case decision making brings a number of challenges. This is true for all evidence and is especially important when research is emergent. 17
- The evidence does not always distinguish between specific forms of abuse and/or neglect, which can be challenging in terms of understanding the distinctive pathways, impacts and required protective actions. It should not be assumed that broad findings are applicable to every form of harm; this review attempts to caution against this but recognises that summary reports of this nature do pose this risk.
- The evidence is sometimes lacking in terms of how specific characteristics, such as gender and ethnicity, interact with the findings on maltreatment or placement type. It is beyond the scope of this review to explore these issues.
- Neither local authority nor judicial decision making take place in a vacuum. There are a myriad of factors that inform professionals’ assessment of whether a child is at risk of significant harm and what is the most appropriate action to take in planning for the child's safety, well-being and future. The messages in this review should be understood within this. The contexts for local authority and judicial decision making are explored below.
1.4 Context for local authority and judicial decision making
The value of using theory and research findings in conjunction with other evidence to inform decision making in child protection and family court decision making has been emphasised in this field in recent years. 18 Decisions are taken at numerous points in the processes where children and families are involved with the judicial system and family courts.
Key points in local authority decision making include, for instance:
- decisions in relation to assessing and responding to the risks, vulnerabilities, protective factors of the birth family and wider network of relationships
- the approaches taken in working with a family to provide support and enable positive change
- providing temporary placements for a child at the parents' request
- complying with the requirements of the Public Law Outline
- ensuring that the child’s right to a family life is taken into account in any plan for the child
- assessing firstly the viability and then the suitability of alternative carers in the family network
- commissioning necessary specialist assessments exploring the provision of a range of alternative placement options as a part of the requirement to make a permanency plan for the child. 19
Theory and research will, implicitly and explicitly, inform professionals’ decision making throughout the child’s journey through the care system and the authority’s recommendations to the court. This may occur implicitly (without direct citation, but underpinning the knowledge and skills which inform the professional judgements made) or explicitly (where research evidence is directly cited to support the analysis made).
Behind an individual social worker’s presentation of a local authority’s recommendations in court are a plethora of other professionals in roles which influence, guide or direct decision making. These professionals commonly (but not exclusively) include: line managers and supervisors; Child Protection Conference Chair; Independent Reviewing
Officer; Legal Advisor; Case Progression Manager; Finance Manager; Head of Service or equivalent. The views of the parent(s) and child should be listened to and considered throughout the process, as should the opinions and advice of other key professionals (e.g. in health, police and education).
During court proceedings, decision making is further influenced by the Cafcass children's guardian, the parent’s lawyers, independent assessors and potentially others. Within the court arena, decision making is informed by negotiations between parties to reach an agreement that is in the best interests of the child.
Judicial decision making is framed by the bedrock principle of judicial independence. Individual judges, and the judiciary as a whole, are impartial and independent and focus on the application of the law to the individual case before them, according to the principles of justice. This ensures that those who appear before them (and the wider public) can have confidence that any decisions are made fairly and in accordance with the law. 20 Judicial independence in the family courts is enacted through each judge deciding cases solely on the balance of evidence presented to the court and according to both statute and case law. In all cases, the welfare of the child is the court's paramount concern. In order to achieve this, key issues are considered by the court:
- The Children Act 1989 requires the court to have regard to the welfare checklist set out in section 1 of the Act when it considers any questions relating to the upbringing of a child. 21
- Any decision in relation to the child is proportionate and balances the various options open to the local authority and the court.
- Under the Children Act 1989 the court is required to take the least interventionist approach. Under the Adoption and Children Act 2002, 'the court must not make any order under this Act unless it considers that making the order would be better for the child than not doing so'. Additionally, parental consent to adoption can only be dispensed with if either parent is incapable of giving consent or the child’s welfare requires this. 22
The legal context for decision making is discussed further in section 4 of this report.
1.5 The evidence review
The bodies of literature pertinent to the topics at hand in this paper are extensive (although there are still gaps in knowledge), cross a number of disciplinary fields, and are constantly being added to with newly published studies. The scope of this review does not enable a definitive summary of all of this material – which would run to several hundred pages. The following sections provide a summary of consistent findings from evidence reviews and research studies on the potential impact of abuse and neglect for children and the potential strengths and weaknesses of different placement options. Gaps in the existing evidence base are also identified.
2. Defining and identifying abuse and neglect
Key points
- Abuse and neglect can occur at different ages and stages of child and adolescent development, and for a multitude of different reasons including a variety of parental vulnerabilities.
- Children and young people's ability to rebound from such adverse experiences is related to a number of characteristics and supporting factors such as their age, family environment, social networks and the wider community.
- Neglect is the most prevalent form of maltreatment; however, it can be difficult for professionals to identify neglect and to evidence whether the threshold for statutory social work intervention and/or court action has been reached. Neglect also often occurs in the context of other factors.
- Individual, community and societal factors interact in complex ways to increase or decrease the risk and impact of maltreatment.
- There are protective factors that can be enhanced and promoted. Providing earlier, effective support to parents, whilst keeping the child's welfare in mind, can reduce the risk of maltreatment.
- Children with disabilities appear to be one group at heightened risk of experiencing maltreatment.
2.1 Safeguarding children
If there is reasonable cause to suspect that a child is suffering, or is likely to suffer, significant harm a local authority has a duty to make enquiries under section 47 of the Children Act 1989 and decide whether any action should be taken to safeguard and promote the child’s welfare .23 Local authorities need to provide factual evidence to the court in order to show that, on the balance of probabilities, a child has suffered, or is likely to suffer, significant harm. Harm is defined in the Children Act 1989 as 'ill-treatment or the impairment of health or development including, for example, impairment suffered from seeing the ill-treatment of another' (s.31(9)). Working Together (2015) 24 provides definitions of different types of harm, including physical abuse, sexual abuse, emotional abuse and neglect (see Appendix 2).
Child abuse and neglect are often subsumed under the umbrella term 'child maltreatment' which has been defined by the World Health Organisation as:
All forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligent treatment or commercial or other exploitation, resulting in actual or potential harm to the child’s health, survival, development or dignity in the context of a relationship of responsibility, trust or power. 25
Whilst acknowledging that there are distinctive characteristics between abuse and neglect, the term 'maltreatment' is used throughout the report where the evidence does not distinguish between specific forms of abuse and/or neglect. Maltreatment can occur at different ages and stages of child and adolescent development.
2.2 Risk factors associated with child maltreatment
Parental vulnerabilities
There are a number of parental vulnerabilities that can have an adverse impact on parenting capacity. It would be incorrect to assume a direct causal relationship between parental vulnerabilities and children experiencing abuse and neglect; many parents who experience some of these issues raise their children safely. Nevertheless, research suggests a heightened risk of child and adolescent maltreatment, in particular where more than one of these factors co-occur, as is often the case. 26 These factors appear to interact with one another, creating cumulative levels of risk and need the more factors are present. Parental factors associated with increased risk of maltreatment of children include:
- parent's exposure to adverse experiences during childhood (e.g. parental domestic violence, substance misuse, mental health issues)
- domestic abuse, mental health difficulties, drug and alcohol misuse (combined or singly)
- a history of crime (especially for violence and sexual offences)
- patterns of multiple consecutive partners
- acrimonious separation
- parental learning disability
- intergenerational cycles of child maltreatment. 27
Where a parent has their own vulnerabilities, such as those listed above, the stresses of parenting are likely to be significantly greater. However, as mentioned, parents facing these difficulties can and do raise their children safely. Although some children who are exposed to parental mental illness, learning disability, substance misuse or domestic violence exhibit behavioural or emotional problems, others show no long-term disorders. 28 Woolgar (2013) has used the term (from developmental science) 'differential susceptibility' to explain why some children are more affected by their earlier experiences than others. It highlights differences in children's sensitivity to positive and negative environments, with some children being particularly vulnerable to relatively low levels of adversity while others are less affected by such environments.
Children’s experience of domestic violence in their home environment is recognised as a form of harm in itself. 29 The impacts of domestic violence on children differ by developmental stage, but when children experience domestic violence in addition to other forms of abuse and neglect there is understood to be a high risk of emotional and psychological harm. 30
It has been argued there is a tension between the need to keep children safe in situations where there is domestic violence and not blaming and/or punishing the non-abusing parent. As noted in a recent report by Women's Aid: 'Every point of interaction with a survivor is an opportunity for intervention. It should not be missed, and should never add to the huge barriers survivors already face … Supporting the non-abusing parent is likely to improve the safety and well-being of children and should always be fully explored.' 31
Understanding the experiences of children and young people in families where there is risk of maltreatment requires direct engagement that goes beyond seeking to understand wishes and feelings (which is itself vital). Social workers must identify and have a nuanced understanding of the daily lived experience of the child. They must also maintain a focus on individual children because similar behaviours on the part of the carer may affect individual children in the family differently 32 and, in some cases, one or more children may be treated differently or experience ‘preferential rejection’. 33
Community and societal factors
Although much of the evidence base on risk factors associated with maltreatment focuses on risks at the individual parental level, the literature also recognises the interaction between individual, community, and societal factors. A recent review of the international evidence found an association between families' socio-economic circumstances and the chances of their children experiencing maltreatment and/or of maltreatment being identified. 34
It is important to note that poverty in itself is not a sufficient factor in predicting the occurrence of maltreatment. Children whose families are not living in poverty also experience maltreatment, just as most children in families living in poverty do not experience maltreatment. Nevertheless, evidence suggests that the direct and indirect impacts of poverty interact in a complex manner with other factors that affect parenting and can increase the risk of child abuse and neglect. 35
Emerging evidence also points to significant inequalities in rates of children's services interventions, which have been found to be linked to deprivation. 36 Research based on a large longitudinal UK cohort study, the Avon Longitudinal Study of Parents and Children (ALSPAC), found that poverty was a significant factor both for investigating child maltreatment and for placing children on child protection plans. Poverty also interacted with other factors in the parental background and family environments. 37 Another UK study tracing the life pathways (from birth to age eight years) of a small group of children (n =36) who were identified as likely to suffer significant harm before their first birthday also found that poverty, unemployment, poor housing, isolation, living in dangerous or hostile neighbourhoods, and parental physical and mental health problems all increased the stressors in families and made the recurrence of factors associated with child maltreatment (e.g. domestic violence, substance abuse) more likely. 38
As with parental vulnerabilities, the relationship between these community and societal factors and child maltreatment should not be understood as straightforward or causal.
2.3 Protective Factors
Individual children and young people's ability to cope with and rebound from adverse experiences is related to a number of characteristics and supporting factors. These include factors such as their age and developmental stage, the presence of resilience- promoting relationships in their lives and access to wider family support. 39 These factors can buffer children from the impact of abuse and/or neglect, and as with risk factors, they can interact with each other.
The welfare of the child is the fundamental concern for social workers and other professionals. However, in addressing the child’s welfare they must also give due attention to the needs and concerns of parents, who may themselves be vulnerable.40 A growing body of research and practice innovation advocates holistic approaches to working with families, which do not compromise the safety of the child and engage parents and wider family in change processes that may help protect their children. 41
Although protective factors have arguably not been studied as extensively or rigorously as risk factors, there is evidence that the following factors can help to protect children from the impact of maltreatment:
- Supportive family environment and social networks
- Communities that support parents
- Adequate housing
- Access to health care and social services
- Nurturing parenting skills
- Stable family relationships
- Reasonable and consistent household rules and child monitoring
- Parental employment
- Caring adults outside the family who can serve as role models or mentors
- The presence of a non-abusive partner
- Parents' recognition of the problems
- Parents' willingness to engage with services. 42
Actions to promote protective factors should be taken as early as possible. One clear premise for providing evidence-informed early help to families is to mitigate the risks of children being maltreated by addressing issues before risks escalate. Messages on effective early help suggest that this relies on reciprocal working relationships across agencies (e.g. between children’s and adult services, including mental health, drug and alcohol, and probation services) and should include ongoing, tiered packages of support (as opposed to bursts of intensive, short-term interventions followed by withdrawal of support) designed to meet the needs of individual children and their families. 43
If intervention and support does not result in sufficient change to protect children from significant harm, then escalation may be necessary. In some cases this may lead to court proceedings and for some children, it will be deemed necessary to remove them from home and into an alternative placement. 44
2.4 Prevalence of abuse and neglect
There are no definitive figures on the number of children who have experienced abuse and/or neglect. Knowledge about the scale of maltreatment in the UK comes from three specific sources:
- recorded offences
- child protection systems
- self-report studies. 45
All have their limitations and estimates vary according to the source of information, the time-period over which data are collected and the ways in which abuse and neglect are defined.
Statistics on recorded abuse and neglect are considered under-representative of children and young people’s experiences. 46 However, evidence from a large-scale 47 self-report NSPCC survey (conducted in the general population in 2009) found that neglect is the most commonly reported form of maltreatment in the family.48 The study found that ‘severe’ child maltreatment49 in the family was reported as an experience for a minority of children and young people during their childhood, as illustrated in Table 1 below.
Table 1: Rates of self-reported severe maltreatment in the family during childhood 50
|
Maltreatment type |
Under-11s |
11-17s |
18-24s |
|
Severe neglect |
3.7% |
9.8% |
9.0% |
|
Severe physical violence |
0.8% |
3.7% |
5.4% |
|
Contact sexual abuse |
0.1% |
0.1% |
0.9% |
|
All severe maltreatment |
5.0% |
13.4% |
14.5% |
More recently, a large national survey of adults resident in Wales (n=2,028) investigated the self-reported prevalence of a range of adverse childhood experiences (ACEs) 51 (verbal abuse; parental separation; physical abuse; sexual abuse; domestic violence in the household; parental alcohol and drug abuse, mental illness and incarceration).
Respondents provided anonymous information on their exposure to ACEs before the age of 18 years and their health and lifestyles as adults. Table 2 summarises the findings from this study. 52
Table 2: Proportion of adults in Wales who reported having been exposed to ACEs
|
Type of ACE |
Prevalence (%) |
|
Child Maltreatment |
|
|
Verbal abuse |
23 |
|
Physical abuse |
17 |
|
Sexual abuse |
10 |
|
Child household included: |
|
|
Parental separation |
20 |
|
Domestic violence |
16 |
|
Mental illness |
14 |
|
Alcohol abuse |
14 |
|
Drug use |
5 |
|
Incarceration |
6 |
The report notes that for every 100 adults in Wales, 47 have suffered at least one ACE during their childhood and 14 have suffered four or more. However, it is important to note that not all ACEs are associated with child maltreatment.
Statistics provided by local authorities via the children in need census (and aggregated by the Department for Education in annual returns) provide data on children referred to and assessed by children's social care services. These show that in the year ending 31 March 2016, 172,290 children and young people in England became the subjects of section 47 enquiries 53, an increase of 7.6 per cent over the previous year. Around 30 per cent of these children (50,310) became the subjects of child protection plans. 54 The most common ‘initial category of abuse’ for children who were in need and who became the subject of a child protection plan is neglect, as illustrated in Table 3 below. 54
Table 3: Initial category of abuse recorded
|
Initial category of abuse |
Per cent |
|
Neglect |
46 |
|
Emotional abuse |
35.3 |
|
Physical abuse |
8.3 |
|
Sexual abuse |
4.7 |
|
Multiple |
5.5 |
Both government statistics and findings from the NSPCC study identify neglect as the most prevalent form of maltreatment. Because of its prevalence, and in recognition that conflating abuse and neglect can be problematic in terms of defining an effective response, neglect is considered in further detail below.
2.5 Neglect
Neglect is a serious and pervasive form of maltreatment that occurs across childhood and adolescence with potential long-term consequences across the life span. Babies and young children are particularly vulnerable and dependent, which makes them especially fragile and places them at higher risk of abuse and neglect and adolescents have also been highlighted as particularly vulnerable. 55 Neglect has also been found to be the most likely form of maltreatment to recur. 56 There are different types of neglect (see Appendix and these can occur together and/or with other forms of maltreatment (e.g. emotional, physical and/or sexual abuse). 57
Identifying neglect and determining whether statutory thresholds for action have been reached can present real challenges. 58 The following characteristics of neglect may make it harder for professionals to recognise that a threshold for action has been reached:
- The chronic nature of this form of maltreatment (as set out in the statutory definition) 59 can mean that professionals become habituated to how a child is presenting and fail to question a lack of progress.
- Unlike physical abuse, for example, the experience of neglect rarely produces a crisis that demands immediate, proactive and authoritative action, making it difficult to evidence that the threshold is met at a specific point in time.
- Neglect can in some cases be challenging to identify because of the need to look beyond individual parenting episodes and consider the persistence, frequency or pervasiveness of parenting behaviours, which may make them harmful and abusive.
- Practitioners may be reluctant or lack confidence to make judgements about patterns of parental behaviour, particularly when these are deemed to be culturally embedded or associated with social disadvantages such as poverty or when the parent is a victim in their own right.
- The child may not experience neglect in isolation, but alongside other forms of abuse. 60
A recent evidence review reports a number of social and environmental factors that are associated with neglect. 61 These include:
- Poverty: Child neglect is more often associated with poverty than other forms of child abuse (although it must again be noted that the majority of poor families do not neglect their children). Poverty can lead to social isolation, feelings of stigma, and high levels of stress. Pervasive stress can make it difficult for parents to cope with the psychological, physical and material demands of parenting.
- Poor living conditions: Neglect is often associated with having poor living conditions. Poor living conditions include: an unsafe home (e.g. cluttered home, holes in the floor, broken windows, exposed wires, leaky roof, infestation of rodents/insects, fixtures and appliances that are broken or not working); overcrowding; and instability (e.g. frequent moves, homelessness, short stays with friends/family, stays in shelters). It is important to bear in mind, however, that neglect also occurs in households with good living conditions but where parents are physically and emotionally unresponsive.
- Social isolation: Parents who neglect their children have, or perceive themselves to have, fewer individuals in their social networks and to receive less support than other parents. This may exacerbate other parental vulnerabilities (see section 2.2).
- Men: Most of the evidence around neglect relates to mothers rather than fathers. Men can be a source of risk and a source of protection to children they are raising. 62 Fathers can be overlooked in assessment in child protection. 63
Some characteristics of young children are also associated with elevated risk of neglect. This is especially the case for babies born before term, with low birth weight, or with complex health needs and disabilities.
2.6 Risk of maltreatment for children with disabilities
There is a growing body of evidence on the increased risk of maltreatment for children with disabilities. #dummy requires link A recent evidence review, based primarily on research from the United States, suggested that there is an association between child disability and all forms of maltreatment. Children with particular impairments, including communication difficulties, sensory impairments, learning disabilities and behavioural disorders, appear to be at heightened risk. The review also found that children with disabilities may experience multiple kinds and episodes of abuse. 65 Although there is an association between disability and child maltreatment, it is not clear whether the maltreatment a child has suffered contributes to their disability or whether their disability puts them at higher risk of maltreatment. 66
The proportion of children in England who are disabled is a contested issue, partly because of differing definitions and sources of data. 67 Children who are disabled do not form a homogenous group, either in severity or type of disability nor in their life experiences. So an understanding of the nature of any disability and how a child’s development is affected are essential in order to appreciate the nature and impact of any maltreatment a child may be experiencing. 68
Disability was a feature in 12 per cent (21 of 178) of cases in the triennial analysis of serious case reviews 2011-14. Cases in the 2011-14 review (and previous reviews) have highlighted the risk of harm going unrecognised, with families sometimes presenting as loving and cooperative. For children of all ages, there was a tendency to see the disability more clearly than the child, with some professionals accepting a different and lower standard of parenting for a child with a disability than would be tolerated for a non- disabled child (e.g. keeping a child shut in the bedroom for 'safety'). 69
A number of reasons for the increased risk of maltreatment for children with disabilities have been proposed, including:
- Individual and societal attitudes and assumptions that are discriminatory and stigmatising. These include a reluctance to believe children with disabilities are abused, and minimising the impact of abuse.
- Professionals not recognising the signs of abuse or neglect. Behaviours indicative of abuse (e.g. self-mutilation and repetitive behaviours) may be misconstrued as part of a child’s impairment or health condition.
- The children's dependence on a wide network of carers and other adults to meet their medical and intimate care needs, which create increased opportunities for maltreatment.
- Communication barriers, which mean that children with disabilities may have difficulty reporting worries, concerns or abuse. Professionals may also fail to consult them and to listen to their experiences.
Professionals' reluctance to challenge carers, together with a sense of empathy with parents/carers who are under considerable stress. 70
Parents of children with disabilities may also experience difficulties (e.g. depression) and isolation as a result of caring for their child. This is sometimes compounded by the lack of consideration given to the impact of the child's disability on family functioning and economic status (e.g. as a result of having to give up work to care for a child), as well as lack of support from statutory services. 71
3. The impact of maltreatment on children and young people
Key points
- Abuse and neglect can have a negative impact on a range of outcomes for children and young people. However, every child is unique and has his or her own susceptibilities and resiliencies. The impacts of exposure to maltreatment vary in relation to factors such as the age at which it is experienced; the intensity, frequency, duration and type of maltreatment; and the individual characteristics of the child.
- It is not possible to predict specific outcomes for individual children based solely on research findings. However, some findings are consistent across research studies. This indicates they should be taken into consideration when making decisions about children's welfare in the immediate term and into the future, alongside critical and analytical observations and assessments of individual children and their circumstances.
- There is strong evidence to suggest that maltreatment is associated with social, emotional, behavioural and mental health difficulties, which can continue throughout childhood and beyond. Although this can have an impact on educational achievement for some children, being at school can also act as a buffer against the negative consequences of maltreatment.
- The mechanisms for these negative outcomes are not fully understood, but may be linked in part to the development of disorganised attachment behaviours in infancy and/or in part to the body's physiological response to the maltreating environment.
- Positive changes to the caregiving environment – specifically, the provision of nurturing, stable and consistent care – can help children recover from the negative consequences of maltreatment.
- Support for carers is crucial both to help them understand the impact of maltreatment on the child's behaviour and so to assist with the child’s recovery. Children and young people may also need specialist support to help them recover from early trauma.
3.1 Introduction
Although research investigating the impact of child abuse and neglect is extensive in some areas, it is difficult to make direct causal links between specific types of experience of abuse and neglect and specific adverse outcomes for children. Many research studies do not control for other adverse environmental and social factors such as socio-economic disadvantage, disability and social isolation. Other research limitations include: problems with definitions of the type and severity of maltreatment (e.g. physical abuse, emotional abuse, neglect); difficulties in recruiting representative samples; and difficulty obtaining accurate recollections of past events by participants. 72
Neglect and abuse occur along spectrums of severity and the evidence suggests that the more chronic the experience, the more marked the symptoms of trauma in childhood and beyond. Impacts may be moderated by various factors including: the child’s age when neglect or abuse commences or occurs; the duration of the maltreatment; availability of protective factors such as sources of nurture and support; individual characteristics in a child’s temperament and genetic characteristics. 73
As previously noted, children have differing susceptibilities and resiliencies to maltreatment; it is not possible to make definitive predictions about the impact of abuse and neglect on children at an individual level. The outcomes for children who are maltreated are determined by multiple factors and 'similar end points can arise from quite different mechanisms and conversely, similar experiences can lead to quite different outcomes '.74 The exception to this is where children suffer severe physical abuse resulting in brain injury or even death (e.g. shaken babies).
Notwithstanding the limitations, research consistently identifies strong links between maltreatment and adverse consequences for children and young people. Local authorities, Cafcass and the judiciary can utilise these findings to inform their assessments and decisions, alongside their professional judgement and expertise.
3.2 The impact of neglect
The impacts of neglect, as with other forms of maltreatment, will vary between individual children. It is with this understanding that the evidence regarding impact should be considered.
Evidence suggests that neglect is a particularly damaging form of maltreatment. Although it can be difficult to disentangle specific effects from those of other forms of maltreatment, there is evidence that for many children neglect has significant implications for a range of developmental dimensions, including health, education, identity, emotional and behavioural development, family and social relationships, social presentation and self- care skills. 75
Neglected infants and toddlers can show a dramatic decline in overall developmental scores between the ages of 9 and 24 months and a progressive decline in cognitive functioning in the pre-school years. In addition, neglected infants who initially display secure attachment behaviours may increasingly develop insecure or disorganised attachment behaviours as they grow older. These findings suggest that the longer young children are exposed to neglect, the greater will be the harm. 76
The experience of neglect in childhood can have long-term impacts on child and adolescent development. For instance, children who have experienced neglect may experience increased vulnerability in adolescence compared to those who have been physically abused 77, potentially increasing the vulnerability of some young people to other types of maltreatment and/or victimisation, such as sexual exploitation (though this is an area requiring further research). 78
In some cases, extreme neglect can be potentially life threatening. The analysis of serious case reviews in England 2011-14 found that neglect was an underlying feature in 62 per cent of the children who suffered non-fatal harm, and in over 50 per cent of the children who died (it should be noted this number is small in relation to the total population of children). Six children aged between four months and just over seven years died over this period directly as a result of extreme neglect (three per cent of all fatal serious case reviews). These children died either as a result of cardiac arrest or multi- organ failure arising from malnutrition. All six were known to children's social care and two were on child protection plans. In all six cases, there was evidence that the family was isolated or that the mother was particularly vulnerable. 79
3.3 Attachment theory and the impact of maltreatment on attachment
Attachment theory
An area where there is relatively broad consensus in the research literature is the adverse impact of child abuse and neglect on the formation of infant attachments. Attachment theory 80 has developed over a number of decades and focuses on the foundational importance of secure and lasting relationships with a caregiver for infant and child development. It should be noted that, whilst attachment theory is widely drawn upon in work with children and families, it is also subject to some critique particularly in relation to methodological issues and causality, and therefore continues to evolve. 81
Security of attachment refers to the degree to which a child has internalised experiences based on relationships with significant others who are perceived as trustworthy, available, sensitive and loving. Early attachment is important because it enables children to learn to trust, develop empathy for others and feel secure knowing that their primary caregiver/s will meet their needs. It is also believed to act as an ‘internal working model’ (or template) for subsequent relationships. 82 Attachment security is also important in adolescence and exerts a similar effect on development as it does in early childhood: a secure base fosters exploration, independence and the development of cognitive, social and emotional competence. 83 Parents’ own attachment patterns (developed, attachment theory suggests, through their experiences of early childhood) also influence parenting capacity, but do not define it. 84
Attachment theory identifies a number of ‘attachment patterns’ which develop through early parent-child interaction, whatever the quality of that interaction, and including in the context of maltreatment. Appropriate and sensitive parental attunement and responsiveness give rise to secure attachment. A consistent and emotionally available caregiver comforts the child and provides a secure base when the child is anxious or distressed. Secure and insecure (i.e. avoidant or ambivalent) attachment are termed ‘organised’ attachment patterns; each is a consistent and predictable way for children to keep carer(s) nearby. Insecure attachment is very common, with an estimated 60/40 split between ‘security’ and ‘insecurity’ amongst the general population. Although it is not optimal, and children may benefit from support and more sensitive parenting, insecure attachment is not in itself cause for alarm. 85
Children who have a secure attachment are generally able to turn to and be comforted by their caregivers when distressed and to use them as a 'secure base' for exploring their environment. Children who have an ambivalent attachment pattern tend to 'up-regulate' their attachment behaviour to maintain proximity to their carer, becoming very distressed when separated and not easily being calmed when comfort is offered. In contrast, children who develop an avoidant attachment pattern tend to maintain proximity by 'down-regulating' their attachment behaviour, appearing to manage their own distress and not signalling a need for comfort.
It is important to note that categorising attachment behaviours is complex and is not an exact science. For example, while insecure attachment behaviours may be observed when the child is exposed to a stressful situation (e.g. separation-reunion procedure), they may not display these behaviours all the time. 86
Disorganised attachment behaviours are described in the literature as being a set of fleeting, temporary behaviours, usually only observable when the ‘attachment system’ is activated (e.g. when the child’s sense of safety/security is threatened, such as when they are hurt, unwell or emotionally upset and/or frightened 87). Examples of this behaviour include infants approaching their caregiver but with the head averted, with fearful expressions, or disoriented behaviours such as dazed or trance-like expressions or freezing of all movement. Such behaviours are understood to mean that the infant is not able to resolve their distress within the context of their relationship, either by signalling their anxiety to their caregiver, or by directing their attention away from them. While it cannot be assumed that their presence always indicates maltreatment, research studies have suggested that these behaviours may be observed in between 48 and 80 per cent of maltreated children. Some children (e.g. those on the autistic spectrum, or children who are frightened for their carer, for example when a parent is terminally ill or subjected to violence) can exhibit disorganised attachment behaviours in the absence of maltreatment. Conversely, it is possible for children who are maltreated not to show disorganised attachment behaviours. 88
The attachment behaviours described above are different to an attachment disorder, which is a formal psychiatric diagnosis outlined in DSM-5. 89 The term 'attachment disorder' is prone to overuse or misuse by practitioners without appropriate psychiatric qualifications to diagnose. 90
Attachment disorder refers to a highly atypical constellation of behaviours indicative of children finding it extremely difficult to form close attachments. Reactive attachment disorder refers to a consistent and pervasive pattern of extremely withdrawn behaviour, with a marked tendency to not show attachment behaviour toward others, accompanied by a general lack of responsiveness and limited positive affect. Disinhibited social engagement disorder refers to a marked and pervasive tendency to not show appropriate cautiousness with respect to unfamiliar adults and a failure to be sensitive to social boundaries. 91
The criteria for formal psychiatric diagnosis of an attachment disorder is that the child has experienced a pattern of extremes of insufficient care in at least one of the following:
- Social neglect or deprivation in the form of persistent lack of having basic emotional needs for comfort, stimulation, and affection met by caring adults
- Repeated changes of primary caregivers that limit opportunities to form stable attachments (e.g. frequent changes in foster care)
- Rearing in unusual settings that severely limit opportunities to form selective attachments (e.g. institutions with high child to caregiver ratios). 92
The impact of maltreatment on attachment
Attachment behaviours are thought to be adaptations to the quality of the caregiving environment. Although they make sense as a way of coping with impaired caregiving, they may have consequences for later well-being. 93 There is some evidence (though not uncontested) that children who are abused and/or neglected may be at risk of developing attachment patterns or behaviours that can increase the risk of later psychopathology; externalising disorders (e.g. conduct and behavioural problems); and personality disorder. 94 However, variations in infant–caregiver attachment cannot explain all the negative outcomes as parents are not the only important social influences on children's development. Sibling and peer relationships are also important and combine with other parenting behaviour to influence development and future outcomes. 95 Some research notes that application of attachment theory to developmental psychopathology, highlights conceptual and methodological challenges 96; this underlines the importance of not assuming attachment difficulties in childhood will translate to later problems.
Although attachments patterns show some stability over time, they are also open to change as a consequence of changes in caregiving. However, because children with attachment difficulties related to maltreatment are often not used to adults being predictable, kind and nurturing, they may inadvertently reject their carers (e.g. kinship carers, foster carers, adopters, special guardians). The behaviours associated with such attachment difficulties can be experienced as very demanding by carers seeking to offer a secure base and safe home. Thus, carers may need additional input to help them understand the behaviours and to support them in maintaining the placement. 97
3.4 Impact of maltreatment on physiological functioning
Research on the impact of maltreatment on the body's physiological responses and on neurodevelopment is not yet at a stage where definitive conclusions can be drawn regarding the interrelated biological, psychological and social factors involved. It is not possible to predict specific outcomes for children based on their experiences of maltreatment. Some research indicates that some children who have been maltreated will have 'complex and individualised neurodevelopmental problems, which could influence their emotional and behavioural adaptations in a variety of ways'. 98 However, researchers also warn that the generalisability of most of these findings is limited as they are disproportionately reliant on clinical samples, which are not representative of all children. 99 Further research is needed before these findings can be applied with confidence in practice.
Research suggests that maltreatment may have an impact on the body's systemic response to stress. A certain amount of stress is normal for all children in their daily lives; and they have inbuilt systems for identifying and responding to physiological, emotional and social stress, which are also developed through experience. However, some research argues that acute stress experienced over a short period of time can have long- term consequences (e.g. post-traumatic stress disorder), and that chronic stress can have short- and long-term consequences. The various systems in the body adapt to the experience of stress and this may have varying degrees of impact on child, adolescent and adult development (e.g. increase the risk for chronic diseases of ageing, including Type II diabetes and cardiovascular disease). 100 However, care must be taken not to assume that maltreatment will result in these impacts. Care must also be taken not to overlook the impacts of other contextual factors.
Evidence emerging from the use of relatively new techniques such as neuroimaging is limited and evolving, and its application to policy and practice is contested. These techniques have been used, for instance, in studies that suggest a pattern of atypical processing of threat-related cues in children who had been exposed to family violence compared to children who had not experienced family violence. 101
Although physiological dysregulation can have consequences for an individual’s development and well-being, there is increasing evidence to suggest that a change to a high-quality nurturing environment (either through positive parental changes or, where improvements cannot be sustained, through placement with alternative carers) can help to stabilise physiological dysregulation. 102 These findings again emphasise the importance of not adopting a deterministic perspective.
3.5 The impact of maltreatment on social, emotional and behavioural development
Much of the UK evidence on the impact of maltreatment on children and young people’s social, emotional and behavioural development derives from research with looked after or formerly looked after children. Since the majority of children become looked after following abuse or neglect (60 per cent in England in 2015-16) these studies provide proxy measures of the impact of maltreatment. 103
Evidence from a number of UK research studies indicates that many children who become looked after (and are at high risk of having been maltreated) have high levels of emotional and behavioural difficulties, which are associated with poor mental health and educational progress. 104 One of the main measures used to assess children's emotional and behavioural well-being is the Strengths and Difficulties Questionnaire (SDQ) 105, a reliable and well-validated screening instrument that can be completed by older children, parents/carers and teachers. There is a strong predictive relationship between SDQ total scores that are in the clinical range and subsequent psychiatric disorders. 106
Biehal and colleagues' longitudinal study of outcomes for children in long-term foster care and adoption found that over a third of children (38 per cent; n=136) had scores over the clinical threshold for severe emotional and behavioural difficulties, as measured by the SDQ, almost four times higher than would be expected in the general population. Scores were especially high on the scales for hyperactivity, peer problems and conduct disorder (33, 36 and 38 per cent respectively). Boys scored more highly than girls for hyperactivity, but children with learning disabilities scored highly across all sub-scales. 107
One of the limitations of this study is that it was unable to measure children's emotional and behavioural difficulties prior to them entering care. Sempik and colleagues sought to overcome this problem by examining the needs of children (n=648) who had not previously been looked after at the point of entry into care to explore emotional and behavioural problems recorded by social workers and psychologists. Using the threshold of 'problems being of concern to current or previous carers', they found that 72 per cent of children aged 5 to 15 showed indications of behavioural or emotional problems at entry to care, with half showing indications of conduct problems and 22 per cent showing only emotional problems. Almost a quarter of children aged under five at entry to care were identified as having indications of emotional or behavioural difficulties. 108
It is not just the severity of maltreatment that influences emotional well-being, but also the length of time spent in an adverse environment and the number of moves in care. 109 For example, research from the US, looking at 729 children, suggests that placement stability in foster care, independent of children's problems at entry into care, can influence their emotional and behavioural well-being. Children who did not experience placement stability were estimated to have a 36 per cent to 63 per cent increased risk of behavioural problems compared with children who had a stable foster placement, regardless of the child's baseline risk for instability (see section 4.6 for further discussion on placement stability). 110
Given the evidence, every effort should be made, firstly to support parents to achieve positive change, and, where this is not possible, to place children in an alternative, nurturing and stable environment at the earliest opportunity.
3.6 The impact of maltreatment on mental health
There is evidence of a significant association between maltreatment and poor mental health in childhood and later life. 111 A systematic review and meta-analysis of the literature on the long-term health consequences for children exposed to abuse and neglect found evidence to suggest a causal relationship between child maltreatment and a range of mental health issues and other problems including:
- depressive disorders
- anxiety disorders
- eating disorders
- behavioural and conduct disorders
- drug use
- vulnerability to sexual exploitation. 112
A large scale survey (n=2,500) by Meltzer and colleagues between 2001 and 2003 collected data on the mental health of children and young people looked after by local authorities in England (not including those with short-term placements) and compared this with data collected on non-looked after children. The study used both structured and open-ended interviews with parents/carers, young people and teachers. The prevalence of mental disorders was based on a clinical evaluation of the data collected by interviewers using questionnaires designed by the Institute of Psychiatry in London. 113 The findings are summarised in Table 4.
Table 4: Comparison of looked after children with non-looked after children for emotional and behavioural disorders 114
|
|
5-10 year olds |
|
11-17 year olds |
|
|
|
Looked after children |
Non looked after children |
Looked after children |
Non looked after children |
|
Emotional disorders |
11% |
3% |
12% |
6% |
|
Conduct disorders |
36% |
5% |
40% |
6% |
|
Hyperkinetic disorders |
11% |
2% |
7% |
1% |
|
Any childhood mental disorder |
42% |
8% |
49% |
11% |
Conduct disorders contributed to the largest difference in psychopathology between looked after children and non-looked after children. The prevalence of mental disorder was greater among boys than girls (49 per cent and 39 per cent respectively). The study noted that prevalence of mental disorders decreased with the length of time in placement, indicating the mediating effect of moving to a nurturing and stable environment.
These findings are consistent with those from a study comparing psychiatric disorder among looked after children in Britain with disadvantaged and non-disadvantaged children living at home. 115 The study found that looked after children showed elevated rates of emotional and behavioural problems when compared to children who were living in birth families where there was significant social disadvantage (Table 5). The conclusion drawn is that the experience of maltreatment prior to entering care is a key factor in subsequent mental disorders.
Table 5: Comparison of rates of mental disorder among British children aged 5-17 116
|
Category of disorder |
Non- disadvantaged children |
Disadvantaged children |
Looked after children |
|
Any disorder |
8.5% |
14.6% |
46.4% |
|
Anxiety disorders |
3.6% |
5.5% |
11.1% |
|
Post-traumatic stress disorder |
0.1% |
0.5% |
1.9% |
|
Depression |
0.9% |
1.2% |
3.4% |
|
Behavioural disorders |
4.3% |
9.7% |
38.9% |
|
ADHD |
1.1% |
1.3% |
8.7% |
|
Autistic spectrum disorder |
0.3% |
0.1% |
2.6% |
|
Other neurodevelopmental disorders |
3.3% |
4.5% |
12.8% |
|
Learning disability |
1.3% |
1.5% |
10.7% |
It should be noted that these findings are based on data from around 15 years ago. More recent data of this kind is not available, although evidence suggests that the prevalence rates for some mental disorders (e.g. depression and conduct disorders) among young people are increasing. 117
3.7 The impact of maltreatment on educational achievement
Social interaction with caregivers and others is crucial to the communicative competence of young children, even at the pre-verbal stage of development. Maternal warmth, acceptance and responsiveness have been found to be positively correlated with the development of communication skills. In contrast, research indicates children with early experiences of abuse and/or neglect are at increased risk of delayed or impaired language and communication skills development, which can then have an impact on their social and educational development. 118
The relationship between maltreatment and an increased risk of emotional and behavioural problems is indicative of children being at greater risk of behavioural difficulties in the classroom, which is likely to have an impact on educational achievement. 119 This is supported by research which shows that children with more severe emotional and behavioural difficulties, as measured by the Strengths and Difficulties Questionnaire (SDQ), were generally doing worse at school than those with fewer problems. The correlation between SDQ scores and poor educational progress was strongest for those with high scores on the SDQ hyperactivity scale. 120
It is important to note that comparing the academic achievement of a group of maltreated children with results for the general population does not control for other factors (e.g. poverty and deprivation) known to influence educational attainment. However a review of the international evidence supports the notion of a link between maltreatment and academic performance. 121 This evidence review suggests that maltreated children are:
- at greater risk of poor school behaviour
- at greater risk of being the victims of bullying in school
- more likely to have special educational needs
- at greater risk of exclusion from school
- more likely to be absent from school. 122
Evidence from a study that used data from the National Pupil Database (NPD) and the data on Children Looked After in England (SSDA903) found that educational progress was dependent on a number of factors, including age at entry to care and the length of time in care. Detailed findings from this study can be found in section 5.5. 123
There is also evidence to suggest that parental vulnerabilities such as substance misuse and domestic violence can negatively affect children's cognitive development and educational achievement. This is thought to be a consequence of:
- the parents' problems dominating the child's thoughts and affecting his or her ability to concentrate at school
- difficulties in attending school regularly because they need to take care of themselves, their parents or siblings
- disruption to schooling because of families having unplanned moves. 124
However, research also shows that children whose parents have these problems do not always have problems at school, and that school can offer respite and a safe haven from troubled home circumstances. 125
3.8 Impact of maltreatment in utero
Many children who enter care have been exposed to maladaptive environments prenatally (e.g. through drug and alcohol abuse). The adverse impact of alcohol misuse during pregnancy is widely accepted and can result in irreversible neurological and physical abnormalities. 126 Excessive alcohol use during pregnancy is associated with an increased risk of miscarriage and can cause Foetal Alcohol Spectrum Disorder (FASD). Symptoms of FASD include:
- stunted growth
- distinct pattern of facial features and physical characteristics (if alcohol is abused during the first trimester when the facial features are formed)
- central nervous system dysfunction. 127
However, there are challenges in examining the impact of drug misuse on foetal development and the longer-term impact on children’s development because mothers often use multiple substances and may also have a poor diet and limited access to antenatal care, which can also affect foetal development.
The effect of substance misuse on the developing foetus is thought to be dependent on three interrelated factors:
- the pharmacological composition of the drug
- the gestation of pregnancy
- the route, amount and duration of drug use. 128
Exposure to domestic violence can also adversely affect the unborn child as a result of physical damage to the foetus through punches or kicks to the abdomen 129 and also, it is suggested, through the impact of maternal stress on the developing foetus. 130 While domestic violence can start in pregnancy for some women, it is more likely to occur where there has been violence pre-pregnancy. Although pregnancy is potentially a time of increased vulnerability for some women, it can also offer protection for others as they may be more likely to be motivated to seek and engage with support at that time. 131
3.9 The impact of maltreatment experienced during adolescence
Adolescence is a concentrated period of physical, hormonal, social and emotional change. It is also a time of increasing independence, exploration and establishing boundaries. This is part of normal adolescent development. For some young people, however, it can be a time of heightened vulnerability and exposure to maltreatment. Adolescents who are navigating the transition to adulthood without a supportive home environment, and young people with early experiences of abuse and neglect, are at increased risk of experiencing more complex and challenging problems at this developmental stage. 132 Adolescents are more likely than younger children to suffer abuse outside of the family. They may become ensnared in behaviours that exacerbate their risk of harm (e.g. substance misuse, going missing from home or school) and they may be incorrectly assumed to be making unconstrained ‘choices’, which means their vulnerability can sometimes be overlooked. 133
Parenting that is neglectful or abusive (at any stage in a child's development) is associated with a range of negative outcomes for young people in the longer term, including: poor mental health and well-being; behaviours that present heightened risk to health (e.g. drug and alcohol misuse); poor academic achievement; antisocial behaviour; offending; and suicide or self-harm. Once again it is vital to note that these associations cannot be taken to indicate causal links between neglectful parenting and negative outcomes. There is also some evidence of reciprocal links; for example, young people’s involvement in offending may put a strain on their relationships with parents and cause parents to disengage. 134 As noted in previous sections, these harms and vulnerabilities tend to interact in complex ways, with some young people experiencing a range of harms that compound each other and can be further compounded by ineffective service responses. 135
There is relatively little research on the maltreatment of adolescents and its consequences, although the work of Stein and colleagues provides working definitions and analysis on neglected adolescents. 136 There is a small amount of research that has explored the relative outcomes for children and young people who are maltreated at different ages. These studies suggest there may be distinctive outcomes according to the age at which maltreatment occurs, with an increased risk of earlier experiences of maltreatment leading to internalising problems at a later stage, and later experiences of maltreatment potentially leading to a wider range of negative outcomes, including behaviour towards others. 137
The triennial analysis of serious case reviews for 2011-14 found that neglect featured prominently in the experience of adolescents at the centre of serious case reviews. Analysis of these reviews suggested that the impact of maltreatment (both abuse and neglect) over time on these young people was not acknowledged by some of the professionals working with them. In some cases, the young person was wrongly seen as being resilient because they were articulate and troublesome. 138 This tendency for young people to be seen as ‘streetwise’, resilient and troublesome (rather than troubled), and for their behaviours to obscure their vulnerabilities and strengths, has also been noted by others. 139
3.10 Evidence-based interventions and support for children who have been maltreated
A number of evidence-based programmes have been reported as being effective in improving outcomes for children and young people who have been maltreated (e.g. Multi- Systemic Therapy; Multidimensional Treatment Foster Care; Functional Family Therapy; KEEP – Keeping Foster and Kinship Parents Trained and Supported), although some do not always transfer effectively into the UK context. 140 It is beyond the scope of this report to review the effectiveness of these interventions or the associated barriers and enablers to effective implementation, but at the core of all these programmes is an approach based on working intensively with the child or young person together with their birth or carer family. The programmes share a number of other features including: engagement with the child and parents/carers; developing positive family relationships; promoting pro- social peer relationships; improving parenting skills; and providing clear and consistent behavioural boundaries.
A recent evidence review on the efficacy of 15 of the most well-used and high-profile therapeutic post-adoption support interventions concluded that there were very few robust published studies currently available to provide evidence of the effectiveness of the interventions (including play therapies, therapeutic parenting training, conduct problem therapies, cognitive and behavioural interventions). 141
4. Placements options for children
Key points
- Children and young people enter care for a variety of reasons. The 'right' placement for individual children will depend on a variety of factors. Decision makers need to undertake thorough and analytical assessments to help them weigh up the pros and cons of the different permanence options and to determine which placement will best meet children's needs through the whole of their childhood and beyond.
- Where children and young people are not able to remain safely with their parents, decisions around securing stable long-term placement should be made at the earliest opportunity as lengthy waits in temporary care and placement moves can have negative consequences for children.
- Placement stability is a key element of permanence. There are a number of interrelated factors that have an impact on stability, including: the age of the child when they enter care; the severity of social, emotional and behavioural difficulties; having a carer who is sensitive, tolerant and resilient; having a carer who can promote the child's sense of identity.
- Siblings are an important part of a child's identity. There are generally clear advantages to placing siblings together, but this is sometimes not achievable and sometimes not desirable. Decision makers need to consider the benefits and detriments of sibling placements for individual children, and, if children need to be separated, have a plan for contact wherever it is safe to do so.
- The benefits and detriments of contact with birth relatives will depend on a variety of factors related to both the child and the relatives. Of particular importance is the quality of contact and the benefits for the child or young person. Crucial to any decision regarding contact is the child's welfare and their expressed views and experiences of contact.
4.1 The legal context for care proceedings
Section 31 of the Children Act 1989 sets out the legal basis (the threshold criteria) for the court to make an emergency protection order 142, care order, or supervision order. A court 'may only make a care order or supervision order if it is satisfied:
- that the child concerned is suffering, or is likely to suffer, significant harm; and
- that the harm, or likelihood of harm, is attributable to —
- the care given to the child, or likely to be given to him if the order were not made, not being what it would be reasonable to expect a parent to give to him; or
- the child’s being beyond parental control' (s.31(2)).
When a court considers any question relating to the upbringing of the child it will consider:
- 'the ascertainable wishes and feelings of the child concerned (considered in the light of his age and understanding)
- his physical, emotional and educational needs
- the likely effect on him of any change in his circumstances
- his age, sex, background and any characteristics of his which the court considers relevant
- any harm which he has suffered or is at risk of suffering
- how capable each of his parents, and any other person in relation to whom the court considers the question to be relevant, is in meeting his needs
- the range of powers available to the court under this Act in the proceedings in question' (s.1(3)).
It is important to note that courts determine only orders that should be made in a child's best interest, and that they do not determine placements. Local authority decisions about placements are made at numerous stages of the process, taking into account a range of factors such as availability and quality of placements as well as the resource implications of different placement types.
4.2 Permanence decision making
Local authorities are responsible for assessing families that are referred to children's services and meet the threshold for such assessment. Should the threshold be met and safeguarding concerns identified, they have a duty to provide support to address those concerns and meet the needs of the child/young person. 143 Any assessment requires careful analysis of the positive and negative factors in a child's life and a consideration of the interconnecting risk and protective factors in families' lives. 144 Robust assessments and provision of support to parents at the pre-proceedings stage are crucial for ensuring that parents are given the opportunity to make positive changes and for timely decisions to be made for children and young people. These assessments and subsequent care plans, and the evidence from the direct work carried out with families, are all used to inform the evidence that may be presented to the court should the needs of the child not be safely met within the home and family environment. 14 5
A third of children who cease to be looked after return home to their parents or relatives 146 (this includes children and young people who are looked after under section 20 voluntary arrangements that have not been ordered through the court 147); this is one form of permanency. However, a significant proportion of children need alternative arrangements to be made for their care. Care Planning, Placement, and Case Review guidance 148 emphasises the requirement that each child in care has a permanence plan to ensure that he or she can have a secure, stable and loving family to support them through childhood and beyond.
Permanence refers not only to legal and physical permanence, but also health care and education and to the emotional dimensions of stability, such as continuity of relationships, community and personal identity. It is about having a family for life and a sense of belonging and connectedness. 149 At its heart is the quality and continuity of the relationships children build with their carers, regardless of placement type.
The 'right' permanence option for a child depends on their individual needs and circumstances. Local authority and judicial decision makers take into consideration a range of factors when considering placement options. For the local authority and the court, this includes balancing the various options to identify the realistic and best placement to meet a child’s needs and circumstances. The quality and detailed content of that evidence is key to good-quality decision making. It should include analysis of the factors that led to care proceedings and of issues such as: the impact of these factors on child development; parental understanding of the child’s needs and acknowledgement of what needs to change, and an assessment of the parent(s)’ capability to change and meet the child's needs now and in the future; and the suitability of other family members to provide care for the child. Analysis of these factors should be underpinned b
reference to relevant theory and sound research, the aim being robust evidence-informed decision making in the child’s best interests. 150
The objective of permanency planning is 'to ensure that children have a secure, stable and loving family to support them through childhood and beyond and to give them a sense of security'. 151 Identifying the 'right' permanent placement for each child is key to the child’s developmental recovery and progress and to avoiding potential risks, such as
- emotional and behavioural difficulties
- school difficulties
- reinforcement of insecure attachments
- going missing, making them vulnerable to harmful situations
- becoming involved in the criminal justice syste
- struggling to make the transition to adulthood, with higher levels of unemployment, homelessness, criminalisation, addictions, and mental health problems. 152
In her review of evidence on permanence for the Care Inquiry, Boddy (2013) highlighted the importance of 'individual solutions for individual children', and the need to support routes not only to legal permanence, but also to place equal value on other ways of achieving permanence (e.g. support for children and families at the ‘edges of care’, permanent return to birth parents, permanence in shared or full-time care). The aim should be to:
- provide high-quality and stable care
- support children’s sense of identity and belongin
- connect past, present and future through childhood and into adult life. 153
A systematic review of the literature on children and young people’s views of the processes associated with being placed in care found that, overall, they wanted more involvement in decisions made about them. The majority reported that the decision to take them into care had been right; however, there was often little choice about where they would live. Many felt that their views were not always listened to and that they were not able to influence important decisions about their lives. Children and young people stressed the importance of having their individual needs and choices taken into account. 154
4.3 Summary of placement types
Special guardianship and kinship care
When children are unable to live with their birth parents, local authorities are required to explore the possibility of a placement with a relative, friend or other ‘connected’ person (kinship care). 155 Kinship care covers a variety of situations
- private and informal arrangements within the family
- registered private foster care
- local authority foster care with family and friend
- kinship care under special guardianship, child arrangements or adoption orders. 156
There is a crossover between kinship care and special guardianship, as nine out of ten special guardians are related in some way to the child (unrelated foster carers comprise the remaining 10 per cent of special guardians). 157 Special guardianship is a private law order under the Children Act 1989. It was first set out in the White Paper Adoption: A new approach, which set out a number of routes to permanence for looked after children. 158 Special guardianship aims to provide the child with a greater degree of security than other orders (except adoption) by empowering carers and restricting applications for revocation by birth parents.
A special guardianship order (SGO) can be made in care proceedings or as a result of free-standing applications to the court by the child’s carers. 'A court may make a special guardianship order in respect of the child on the application of:
- any guardian of the child
- a local authority foster carer with whom the child has lived for one year immediately preceding the application
- anyone who holds a residence order with respect to the child, or who has the consent of all those in whose favour a residence order is in force
- anyone with whom the child has lived for three out of the last five years
- where the child is in the care of a local authority, any person who has the consent of the local authority
- anyone who has the consent of all those with parental responsibility for the child
- any person, including the child, who has the leave of the court to apply' 159
Although it is applicable in a wide range of situations, it has come to be used, in the main, to secure placements within the extended family network. There are no restrictions on the age of the child but the policy framework originally identified the order’s applicability to older children who were separated from their birth family and were already living with a relative or foster carer. 160
Special guardianship enables a special guardian to exercise full parental responsibility to the exclusion of all others with parental responsibility for a child up to the age of 18. However, there are some limitations on this (e.g. special guardians cannot change a child’s name or live abroad without the court’s consent). Unlike adoption, an SGO does not legally sever the child’s relationship with his or her birth parents and there is an expectation that direct contact with birth parents and other family members will continue if it is in the best interests of the child. While birth parents may apply to the court for a change in contact or in relation to specific issues, they cannot challenge the order itself unless given leave to do so by the court. 161
Adoption
The Adoption and Children Act 2002 and Children and Families Act 2014 provide the framework for decision making with regard to a child being placed for and eventually adopted. This sets out the basis for the local authority to apply to the court for a placement order, which then authorises the local authority to place a looked after child (who is the subject of a placement order) for adoption. 162
'The court may not make a Placement Order under section 21 of the Adoption and Children Act 2002 unless-
- the child is the subject of a Care Order; or
- the court is satisfied that the child is suffering or likely to suffer significant harm; or
- the child has no parent or guardian.
The court may only make a placement order if, in the case of each parent or guardian of the child, the court is satisfied-
- that the parent or guardian has consented to the child being placed for adoption with any prospective adopters who may be chosen by the local authority and has not withdrawn the consent, or
- that the parent’s or guardian’s consent should be dispensed with'. 163
'The court cannot dispense with the consent of any parent or guardian of a child to the child being placed for adoption or to the making of an adoption order in respect of the child unless the court is satisfied that-
- the parent or guardian cannot be found or is incapable of giving consent, or
- the welfare of the child requires the consent to be dispensed with' 164
Adoption severs the legal ties between children and birth parents (although there may be indirect or direct contact) and transfers full parental responsibility to the adoptive parents.
Foster care
Foster care can be short-term (e.g. in an emergency, for respite or assessment), intermediate (e.g. for treatment, preparation for independence or for adoption) or long- term. 165 In 2016 around three-quarters (51,850) of looked after children were placed in foster care at some point, with around one in six being fostered by a relative or friend. 166 A minority of children (320) were in placements where the carer was also an approved adopter (‘fostering for adoption' 167), or where they were subject to concurrent planning (where a child is placed with carers who will foster the child while rehabilitation is pursued with birth parents, and who are prepared to adopt the child should rehabilitation prove unsuccessful).
Long-term foster care can provide children with the security and stability they need until adulthood and is an important permanency option for many children, including those who have a strong sense of identity with their birth family. 168 In 2015, the government introduced changes to Care Planning, Placement, and Case Review guidance to ensure that long-term foster care is considered as a proactive permanence choice for children and introduced measures to improve the status, security, and stability of long-term foster- care. 169
(Although short-term foster care plays a critical role in helping to prepare children for permanence, it is beyond the scope of this review to consider short-term foster care. The focus of this review is on outcomes in long-term placements.)
Child arrangements orders
A child arrangements order is a private law order under section 8 of the Children Act 1989. It was introduced as part of the Children and Families Act 2014 and replaced residence and contact orders. Child arrangements orders determine with whom a child is to live and when, how and with whom a child is to spend time or have contact. Although local authorities cannot make an application for a child arrangements order, it is one of the orders (like special guardianship) that a court can make within care proceedings.
Children's residential care
There has been a renewed policy impetus to improve the quality of children's homes, with new regulations and guidance introduced in April 2015 setting out quality standards that incorporate aspirational, child-focused outcomes. 170 More recently, an independent review of children's homes in England found that the majority of homes visited were providing good care for the children and young people living there. 171 This is consistent with previous academic research on children’s homes, which found that in most homes care was good, but staff turnover was very high. 172
Recent analysis of data on children and young people living in children's homes found that:
53 per cent of children were placed on a voluntary agreement. The majority of the remainder (46 per cent) were placed as a result of care orders.
Most were between the ages of 10 and 15 years (56 per cent) or were aged 16 or over (41 per cent); the average age was 14.6 years.
There were more boys than girls (62 per cent and 38 per cent respectively). 173
There is some evidence to suggest that residential care might offer a preferable permanence option for a small minority of young people for whom fostering is not suitable. 174 This is especially the case for children who do not like living within another family, but who want elements of family life in the home. Children with experience of living in a children's home who contributed to a study by the Office of the Children's Commissioner for England identified that they want:
- to have their views reflected
- to be in a placement that matches their needs
- good staff with whom they can build relationships
- to maintain relationships with their birth family
- have a sense of belonging and the same opportunities as their peers. 175
4.4 Use of different placement types and legal orders
At 31 March 2016, the majority of looked after children (62 per cent) were placed with unrelated foster carers; a further 12 per cent were in a foster placement with a relative or friend. 176 Figure 1 provides a summary of the different placement types for looked after children. It is important when considering the data below to note that not all children who are looked after have been the subject of care proceedings (e.g. children who become looked after under voluntary arrangements and who may or may not enter care at a later stage). As such, the data conflates findings on children who have been the subject of care proceedings with other children who are looked after.
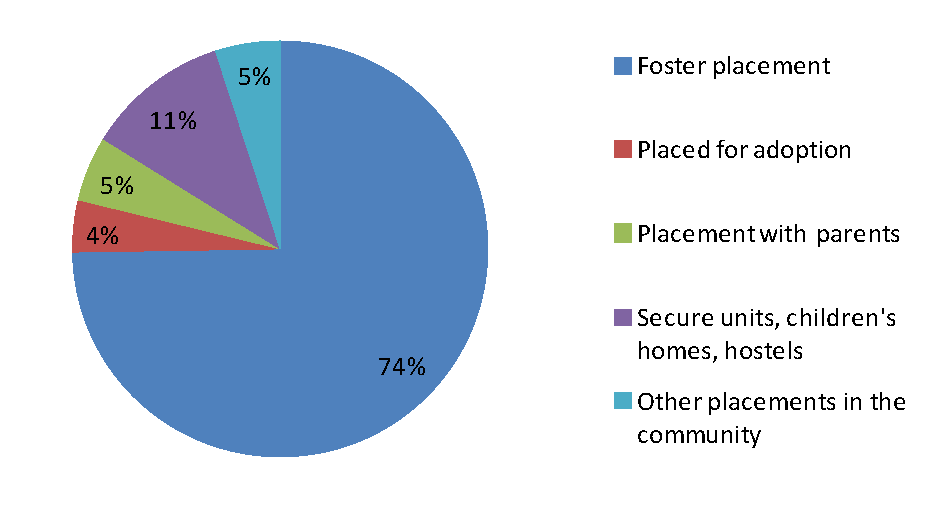
Figure 1: Proportion of children looked after at 31 March 2016 by placement
The highest proportion of looked after children (34 per cent) returned home to live with their family after a period in care (Figure 2). 177 Fifteen per cent of children were adopted and 12 per cent left care following a special guardianship order (SGO) being granted.
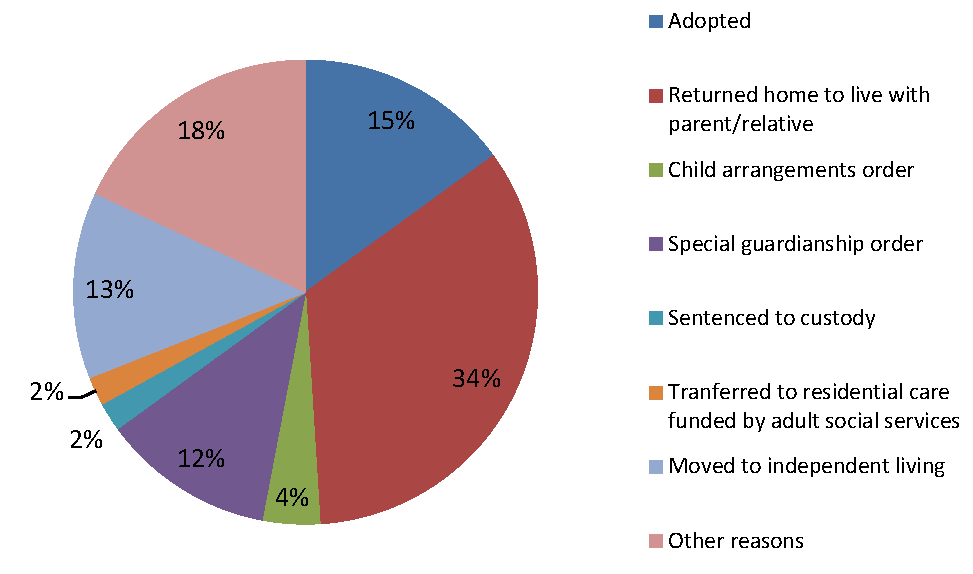
Figure 2: Proportion of children who ceased to be looked after by reason (31 March 2016)
There has been a steady growth in the use of SGOs since their implementation in 2005, with 3,830 children (12 per cent) ceasing care due to an SGO in 2016; this represents an increase of eight per cent on 2015 and a cumulative increase of 78 per cent since 2012. The increase in the use of SGOs has taken place at the same time as the fall in the number of placement and adoption orders. In 2016, 4,690 children (15 per cent) ceased to be looked after due to being adopted. Whilst this is higher than the 3,470 children adopted in 2012, it is less than the 5,360 adopted in 2015, a drop of 12 per cent. 178 Alongside this rise in SGOs, analysis of national data from the Cafcass database has found that there has been an increase in the use of supervision orders with SGOs; in 2014-15 this was 29 per cent, up from 11 per cent in 2010-11. 179
4.5 The characteristics of children in different placements
Although some research studies have compared outcomes across different placement types, few have analysed national administrative data sets to compare the characteristics and outcomes for children in different placement types. One study that has sought to do this is Selwyn and colleagues' study (2014) 180, which analysed administrative data from local authorities (SSDA903 returns, 2000-2011) on over 38,000 children to compare adoption, SGOs and residence orders (ROs, now known as child arrangements orders). This section draws heavily upon this research, as well as research on special guardianship by Wade and colleagues (2014), who used the same data as Selwyn. 181 Although considered to be robust, it should be borne in mind that the findings from this research only relate to data up to 2011, which pre-dates much of the statistics outlined above.
Ages of children at entry to care and at final order
Selwyn's study found that children who were adopted were the youngest at entry to care (average age 1.2 years) compared to children with an SGO (average age 3.4 years) or residence order (RO) (average age 4.5 years). 182 Children who were adopted also tended to be younger at the point of the final order being made compared to children with a SGO or RO, perhaps reflecting their younger age at entry to care (Table 6). 183 However, there has been an increase in the use of SGOs for infants under one year old in recent years, from around 15 per cent in 2010-11 to 30 per cent in 2014-15, with a shift away from placement orders being made for this age group. 184 The ages at which children on different orders enter care is an important factor when considering outcomes for children in different placements as older age at entry to care is associated with placement instability (see section 4.6).
Table 6: Proportion of children in different age groups at the time of the final order (2000-2011) 185
|
Age (years) |
Adoption (N=26,478) |
SGO (N=5,899) |
RO (N=5,760) |
|
0-4 |
71% |
60% |
50% |
|
4-11 |
27% |
34% |
37% |
|
11+ |
1% |
6% |
13% |
More recent national data (2015-16) on the ages of children at the time of the adoption order are provided in Table 7. By way of comparison, Cafcass data showed that 30 per cent of the SGOs made in 2014-15 were for infants under the age of one year. 186
Table 7: Number (and proportion) of children in different age groups at adoption 187
|
Under 1 |
1 to 4 |
5 to 9 |
10 to15 |
Average age |
|
230 (5%) |
3,370 (72%) |
1,020 (22%) |
70 (1.5%) |
3yrs 5months |
Recent research showed that children who were adopted tended to wait longer between entering care and moving into their final placement with their adoptive parents, compared to children who left care through SGOs or ROs. 188 The speed of placement for children on SGOs and ROs is partly attributable to these children being initially placed with kinship carers, who subsequently took out a legal order. The introduction of fostering to adopt and the drive to increase the number of adopters (particularly those willing to adopt older children, sibling groups and children with disabilities) 189 may have reduced the length of time before children are placed with their adoptive parents, but as yet there is no research to confirm this.
Selwyn and colleagues found that 38 per cent of the children who were the subject of SGOs or ROs did not experience any moves in care after their first placement (i.e. they were placed with the relative who became their SGO or RO carer). In contrast, children who were adopted were more likely to have had two or more moves in care before being placed with their adoptive family (although this may have changed following the introduction of fostering to adopt). However, 39 per cent of children with a RO experienced one or more unsuccessful attempts at reunification with their parents, compared to adopted children and those with an SGO (8 and 10 per cent respectively). 190
4.6 Placement stability
A key element of placement stability is identifying the right placement for each child or young person; this involves good assessment, care planning and support packages. 191 Where children are not able to live with their family and need a long-term placement away from home, it is important to 'match' children with alternative carers. Matching is the process of identifying a family who will, as far as possible, meet the assessed needs of a particular child or sibling group, throughout childhood and beyond. 192 The child's emotional, behavioural, attachment and health needs and individual temperament need to be balanced with the carers’ parenting approach and skills. 193
Relational ‘chemistry’ between carer and child is an important factor in stability and permanence for children in permanent placements. Parenting characteristics that help to support children and young people who have been maltreated include sensitivity, boundary setting, tolerance and resilience in the face of behaviour and circumstances that may trigger strong emotional responses. Acceptance and development of new relationships (e.g. through foster care or adoption) may take time for any child, especially those whose previous relationships have been characterised by adversity. Thus, a significant period of adjustment may be needed for both the child and the carers following on from placement either prior to or post any court order. 194
In terms of attachment, children and young people who are removed from their family may experience feelings of loss, even if they have been maltreated. Although not true for all children, when some children arrive in their placement following maltreatment, they will already have established behaviour patterns to deal with distress based on their early experiences. These children are likely to have negative expectations of adults (including social work and other professionals) and may act as if they do not want or need new carers, transferring patterns of behaviour that served to protect them in the maltreating environment into their new environments (e.g. foster or adoptive families). 195
These feelings may be compounded if they experience multiple placements because children need a secure base to establish positive relationships. 196 Where children are not able to remain with their parents, a secure long-term placement at the earliest opportunity is in the best interests of the child, as lengthy waits in temporary care can mean that children are more likely to have multiple changes of carer and suffer additional losses, which they must overcome in order to make a successful attachment to new carers. 197 However, the paramount consideration is the child's welfare, so timeliness needs to be balanced against the need to ensure that the right decision is made for, and with, the child to meet their long-term needs.
Although some children who have been maltreated may find it hard to let adults come close enough to establish trusting relationships, caregiving that is warm, consistent and reliable can change the child’s previous expectations of close adults and of themselves. As previously discussed, a significant proportion of children who have been maltreated have social, emotional, behavioural and/or mental health problems. Families who offer placements need more than good parenting skills to offer the intensive care that some of these children need. They also need to be able to recognise the protective coping behaviours the child has developed and to support the child or young person to move on from these. 198
Another important element of placement stability is identity. Children develop a sense of who they are from birth, based on relationships with family members and others.
Research indicates that some children who are not able to live with their family may have difficulty developing a clear sense of identity. They may also experience a conflict of loyalty between their carer and birth family. Life story work and contact with family members, wherever safe and appropriate, can help children to develop a clearer sense of their identity (see section 4.8). The child's 'new' family also needs to be flexible to give the child space to fit in within the family, which is likely to be very different to the one from which they were removed. 199
Children's sense of integration and belonging in their new family are also important for placement stability and children's well-being. This is discussed further in section 5.
Placement instability
In the year ending 31 March 2016, over two-thirds (68 per cent) of looked after children had one placement during the year, 21 per cent had two placements and 10 per cent had three or more placements (although this data does not separate out children subject to care orders and those in care under section 20 voluntary arrangements). 200 Longitudinal analysis of data on looked after children (conducted in 2013) found that only 17 per cent of all fostered children between the ages of 5 and 18 had been in the same placement for more than five years. 201
Research over the last two decades has demonstrated a strong association between frequent placement moves in foster care and poor outcomes for children. A review and meta-analysis of disruptions in foster care found that older age at placement, behaviour problems and a history of residential care and previous placements showed significant associations with placement breakdown. 202 It is also important to consider the possibility that placement instability may be due to the behavioural and/or emotional difficulties children have prior to entering care. Research from North America has found that placement stability/instability, independent of a child's problems at entry into care, can influence children's emotional and behavioural development. 203
While a stable, permanent placement for a child or young person that will see them into their adulthood is generally viewed as desirable, it must be noted that a placement that is stable but in which a child is deeply unhappy may not be in the best interests of the child. Children and young people may have valid reasons for requesting a placement move or ‘voting with their feet’ and leaving a placement. 204
See section 5 for further discussion of factors associated with placement disruption.
4.7 Placements with siblings
Children who become the subject of care proceedings often come from very complex and fragmented families, which makes decision making for individual children within the same family particularly challenging. Children within the same family may have full- or half- siblings who may either live in the same or different households. 205
The importance of maintaining sibling relationships is recognised in policy and legislation, with an assumption that siblings should be placed with the same carer unless there is good reason not to do so. Saunders and Selwyn’s study (2010) of 14 adoption agencies that had placed three or more siblings with adopters in recent years found that almost half the children were not living together in foster care prior to the adoptive placement.
The main reason for this was the lack of foster carers available for large sibling groups. 206
The Children's Care Monitor (2013-14) found that 63 per cent of children in care had at least one brother or sister who was also in care; of these children with siblings, 71 per cent were separated from brothers or sisters by being placed in different placements. Boys, young people aged over 14, children with disabilities and those living in children’s homes were more likely to be separated from one or more siblings in care. However, 91 per cent of children who had been placed together with their siblings thought this had been the right decision in their case; only 45 per cent of those who had been separated from their siblings thought this had been the right decision. 207
Siblings are an important and integral part of a child’s sense of identity and belonging. They provide support and companionship, have a key role in children’s social and emotional development and are likely to be the most long-standing relationship a child has. Sibling loyalties can be intense, and may be more so where parents have been absent or hostile during the early years. If parents are neglectful, siblings may take over some of the parental roles, which can lead to that child becoming the primary attachment figure for younger siblings. However, not all sibling bonds that develop in traumatic conditions are positive. Sibling caretaking can pose risks as some siblings can be more punitive than parents. Furthermore, children who provide emotional care and developmentally inappropriate responsibilities may be at risk from developing mental health problems. 208
There are times, therefore, when siblings need to be separated – for example, when there are high levels of conflict or abusive patterns of behaviour between siblings. Other reasons for separating siblings include:
- Older siblings not being able to invest emotionally in a new family and hindering the emotional investment of a younger child.
- Harmful sexualised behaviour between siblings.
- Differences in age between siblings, meaning that a care plan for an older sibling may be permanent foster care, while for younger siblings adoption may be in their best interests.
- A relative of one of the siblings offers a home to one child but not the others.
- There are a limited number of families available to accommodate the size and age range of the sibling group. 209
Saunders and Selwyn's 2010 study on adopting large sibling groups found that some of the difficulties in placing children together for adoption were a result of local authorities’ policies and the beliefs of individual professionals. In some cases, social workers believed that placing three or more siblings together would destabilise the placement; however, evidence suggests that the greatest difficulties occur for adopters who have two or more children with serious behavioural problems, rather than having a large sibling group per se. 210
National statistics do not provide data relating to sibling placements. However, an overview of international evidence by Hegar in 2005 suggests that siblings were more likely to be separated in care if:
- the children were older
- there was a large age gap between siblings
- children were of different genders
- children entered care at different times
- some of them had special needs
- placement changes had been more frequent and recent. 211
Although there is research comparing the outcomes for siblings placed together or separately, it is difficult to provide any definitive conclusions as the studies often consider adoption and fostering together, compare sibling placements with those of single children as well as single separated siblings, and include sibling groups under the heading of ‘special needs adoptions’. Notwithstanding these issues, Hegar’s review of the international literature concluded that joint placements are generally as stable or more stable than placement of single children or separated siblings, and that children do as well or better when placed with siblings. 212
Where siblings do have to be separated, it is important that there is a careful assessment of individual children's needs and wishes regarding contact, in order to establish what is in the best interests of a child. While some children may be pleased to see their siblings, this is not the case for others and children in the same sibling group often respond differently to contact visits. 213 The pros and cons of contact are discussed in the following section.
4.8 Contact with birth relatives
Contact for children in care
The Children Act 1989 states that where a child is in the care of a local authority, the authority shall allow a child to have 'reasonable contact' with parents/guardians (s.34(1)).
For children who have recently entered care, contact plays an important role in the assessment of whether return home will be safe as well as being an important part of maintaining significant relationships. The age of the child is an important factor in contact arrangements; for older children or children in long-term foster care, the focus is on preserving or developing existing relationships, while for young infants the main aim is to help the child develop the attachment relationship with (usually) the birth mother, as well as to teach and assess parenting. 214 Maintaining family networks, as part of children's past, present and future identity, is import to ensure that 'children are supported to develop a sense of belonging and identity that addresses the complex and varied meanings of “family” that they have experienced'. 215
There is a strong association between quality of contact and return home, although there is no clear evidence that contact in itself contributes to reunification. Certain factors associated with contact have been found to increase the likelihood of return home: when contact is well planned and resourced; where both parent and child respond well to contact; and where the child's relationship with the parent is positive. 216
Contact for infants subject to care proceedings can be particularly challenging. One study found that contact was frequently distressing for infants, even if it was carefully supervised and supported. Of particular concern was the constant disruption to the infants’ daily routine. 217 Frequent contact arrangements can produce high levels of stress for infants through discontinuity of care and potentially insensitive care during contact, particularly for infants who have experienced unreliable or chaotic care in the past. The distress from frequent and often unsatisfactory contact can add to difficulties in aiding their recovery. 218
(The Association of Directors of Children’s Services and Cafcass have produced a good practice guidance note on contact. 219)
Contact for adopted children
In relation to post-adoption contact, local authorities must balance contact decisions with the need to safeguard and promote the welfare of the child, considering the importance of the relationship with the birth family and the potential for disruption of the placement. The child's welfare is paramount. The purpose and type of contact, and the outcomes for children as a consequence of contact, will differ as a result of a number of complex and interrelating factors and these need to be fully assessed to ensure that the child's needs and best interests are met. 220
Contact with birth relatives after adoption is complex and it is particularly important when considering research findings in this area to take account of the range of situations in which contact can occur, with cases differing according to the age of the child at placement, reason for adoption, child's background and relatives included in the contact plan. 221
Letterbox contact is the most common form of contact between adopted children and their birth relatives. It can provide important information that can answer a child’s questions and show that they have not been forgotten or rejected. 222
Children who are adopted are more likely to have direct contact with siblings than with birth parents, particularly if siblings are placed in other permanent families. This can be a positive experience; when contact with siblings works well (for children placed away from home), there is good interaction and affection and it enables siblings to talk about past trauma with each other. Children are less likely to be in contact with siblings who remain with the birth family. 223
A number of benefits have been identified for children having direct contact with birth relatives. These include:
- continued relationships with birth relatives with whom children have a bond
- reduced feelings of rejection and abandonment
- reassurance that the relative is safe
- help to understand why they were adopted
- help to develop their sense of identity
- help to understand birth parents’ difficulties. 224
However, direct contact with birth relatives does not work well for all adopted children. The following problems with direct contact have been identified:
- children may be unsettled or disturbed by direct contact, particularly if there has been previous maltreatment
- re-abuse during unsupervised contact
- contact with siblings can introduce exposure to negative behaviours
- re-experience of extreme emotional stress
- rejecting or hostile behaviour from birth relative. 225
Neil and colleagues' recent follow-up study of adopted children into adolescence found that just over two-thirds of these 45 adopted young people (aged 14 to 21) still had contact with at least one birth relative, generally once or twice a year. Across time, the majority of contact arrangements had altered in some way, with over half of arrangements reducing in frequency or stopping altogether. Changes in contact were often initiated by adoptive parents as a result of the benefits and challenges they and the adopted young person were experiencing. In some case social media was used by young people, adoptive parents and birth relatives to make contact. 226
Contact for children who are the subject of SGOs
Special guardianship assumes that there will usually be continuing relationships between children, their birth parents and other family members. This is a major strength of special guardianship, but can also be a challenge as the structure and dynamics of family relationships are generally complex and prone to tension and conflict. Relationships within the family can be difficult to manage and there may be concerns regarding children's safety during contact. 227
Wade and colleagues found that many of the children in their study had regular contact with relatives, including at least monthly contact with birth mothers (36.5 per cent), grandparents (31.5 per cent), aunts and uncles (56.5 per cent) and with a wide range of other family members (50 per cent), including siblings, cousins and more distant relatives. However, from the guardian’s perspective, the quality of contact between children and their birth parents was highly variable. In relation to contact with birth mothers, just over half of cases (53 per cent) were considered to have a positive effect on children. Although contact with birth fathers was less common (around one half of the children had no contact with birth fathers, compared to three-quarters of children having contact with their birth mother), where it occurred regularly it was often perceived by guardians to be beneficial (71 per cent). 228
A negative rating for birth-mother contact was more likely where children scored highly for emotional and behavioural problems and when their overall developmental progress was poor. For these children, the fallout from contact tended to exacerbate already existing problems. Where family relationships were positive, contact arrangements tended to be negotiated informally between family members. This was easier where the birth parent accepted the placement and there was a willingness to work together to support the child. In these cases, children experienced fewer signs of distress. 229
Factors associated with beneficial and detrimental contact
A range of factors in the child and in adult birth relatives are associated with beneficial or detrimental contact in permanent placements. These have been identified in relation to adoption and permanent foster care and may or may not apply to special guardianship. Factors associated with beneficial contact are set out in Table 8 and those associated with detrimental contact in Table 9. 230
|
Factors for children |
Factors for adult birth relative |
|---|---|
|
Placed in infancy |
Never been the child's permanent carer |
|
No pre-placement relationship, or positive or neutral relationship with relative |
Accepts and supports the placement, affirms new carers |
|
Absence of major behavioural or mental health problems |
Relinquishes parenting role, where they have been the child’s permanent carer |
|
Secure attachment to current carers, placement provides a secure base |
Relates to the child in a positive, non- abusive way |
|
Healthy psycho-social development |
Relatively free of significant personal difficulties |
|
Child freely wants contact, is not afraid |
Reliable, punctual |
|
Child has positive memories |
Accepts harm caused to child, expresses regret and remorse |
|
Child has not witnessed violence, does not imitate violence |
Does not use contact to undermine, threaten or cause conflict with carers |
|
Factors for children |
Factors for adult birth relative |
|---|---|
|
Insecure attachment and/or unstable placement |
Does not accept or undermines placement |
|
Major behavioural or mental health problems |
Insists on maintaining role as main carer |
|
Rejected, has lived with several birth relatives |
Seriously maltreated child in the past (including through domestic violence towards other parent) |
|
Older child with troubled relationship with birth parents |
Neglectful, abusive or rejecting during visits |
|
Re-traumatised/overwhelmed by contact |
Unreliable, repeatedly late |
|
Child is afraid, feels fearful on return to placement, trust in carers is undermined |
Denies causing harm, shows no regret or remorse |
|
Child does not want contact |
Exposes child to behaviours that are at odds with the placement (e.g. drug misuse, criminality) |
|
Child has negative memories of the birth family |
Significant personal difficulties (e.g. substance misuse, serious mental health problems) |
|
Child has witnessed violence, imitates violence |
|
5. Comparison of outcomes for children in different placements
Key Points
- It is difficult to compare like-for-like outcomes for children in different placement types. However, there are a number of common themes across the research literatures, which provide a reasonably strong evidential base.
- Children in all placement types are equally likely to suffer from a high degree of social, emotional and behavioural difficulties. These are generally more pronounced for children who are older (generally aged four or over) when they enter care. For many children, these difficulties persist even after they have been moved from an adverse environment to a nurturing home, indicating the pervasive impact of lengthier exposure to maltreatment.
- Children who have been maltreated generally have better outcomes with regard to stability and well-being if they are placed in alternative care, particularly if the parental issues relating to maltreatment have not been addressed.
- Purposeful social work planning, which allows children to return home gradually and with the provision of ongoing support, is key to successful reunification.
- Adoption, special guardianship, residence orders/child arrangements orders and long-term foster care all offer permanence options for children who are not able to be reunified with their parents. They also have lower disruption rates than reunification, especially where reunification is not well supported.
- In terms of stability, adoption has a lower rate of disruption compared to SGOs and residence orders. Adoption disruptions are most likely to occur in the adolescent years, after children have been living with adoptive parents for a number of years. In contrast, SGOs and child arrangements orders (formerly residence orders) tend to disrupt within two years of the order being made. Since SGOs were only introduced in 2005, it is too early to say whether a similar peak of disruption as for adoption will occur during adolescence.
- Placements are more likely to disrupt when children enter care and their permanent placement at an older age. So it is important that timely decisions are made where children are not able to remain safely with their parents. These decisions need to be underpinned by robust and analytical assessments of parents and their capacity to change with the provision of support.
- Although there is an association between being in care and educational outcomes, this relationship is mediated by a number of individual, family and environmental factors. The relationship between being in care and low educational outcomes is partly explained by children's pre-care experiences, although some of the difficulties persist once children enter care. Recent research suggests there are positive educational outcomes for children in care in comparison with children in need in the community.
5.1 Challenges in comparing placement outcomes
Research comparing outcomes for children in different placement types can be problematic, making like-for-like comparisons very difficult to establish. Challenges in making comparisons between placement types include:
- Children tend to enter different placements at different ages: research consistently shows that there is a strong relationship between age at placement and disruption, which is likely to have an impact on outcomes.
- There are differences in the length of time for follow-up from a child entering the placement.
- Children have different pre-placement histories, which are often not fully captured in research. For example, many studies do not include a baseline measure of a child's emotional and behavioural development prior to placement; this means it is difficult to make like-for-like comparisons of longer-term outcomes
- Research is conducted at a particular point in time and often utilises historical data. Such data, whilst very helpful, may not capture findings that are relevant in the current policy context.
- Different studies on placement outcomes tend to compare one or two different placement types, making comparison between studies difficult. 231
All of these factors can have an impact on how a placement appears to be affecting a child’s outcomes. The following sections compare outcomes across placement types. Some areas of research (e.g. adoption and special guardianship) have been studied in more depth and been subject to comparison of data than other areas (e.g. residential care); therefore they are presented in more detail than other types of permanent placement.
5.2 Comparison of outcomes: reunification or separation
There is evidence that outcomes for maltreated children who remain looked after are better than for children who return home with respect to stability and well-being, particularly if the issues relating to the maltreatment have not been adequately addressed. Wade and colleagues' 2010 research comprised a census study of 3,872 children who were looked after by seven local authorities, as well as a survey and interviews with a sample of birth parents/carers and children. Outcomes were assessed around four years after the initial decision on whether the child should return home (home group) or remain looked after (care group) and comparisons were made between these two groups. 232
Outcomes for the care group were better than for the home group in a number of ways, including:
- Only one third of the home group remained continuously at home; almost 60 per cent had returned to the care system at least once and one in five experienced more than one attempt at reunification. Children in the care group were more settled, with 65 per cent remaining in the same placement for two or more years, compared to 41 per cent of those who returned home.
- Most children in the care group had settled well, had good relationships and were doing well at school.
- Many felt safer, were relieved to be away from dangerous homes and were well cared for.
- Well-being levels were higher than for those who had remained continuously at home.
- Problems early in reunion predicted poor well-being at follow-up.
- Children who had experienced one or more breakdowns at home fared worst of all.
- Where there was strong evidence of serious emotional abuse or past neglect, children had better outcomes if they remained in care. 233
Children in the group remaining looked after also fared better on a global outcome measure (measuring risky behaviour, emotional and behavioural development, school adjustment) than children who returned home, even where the reunification remained stable. The children who had unstable returns home had the worst overall outcomes. There were often early signs that a reunification would fail; over one third of the children re-entered the care system within six months of returning home. 234
Similar findings have been reported by Farmer and Lutman (2010). In this five-year follow-up study of 138 children who had been neglected and subsequently returned to their parents:
- 65 per cent of the returns home had ended.
- At the two year follow-up, 59 per cent of the children had been abused or neglected after reunification.
- Researcher ratings of the children’s well-being at the five-year follow-up point showed that 29 per cent had good well-being, for a third it was satisfactory, whilst 38 per cent had poor well-being.
Children living stably away from home were more likely to have good overall well- being (58 per cent), whilst for those with unstable outcomes it was most often poor (70 per cent). Children who were stably at home had a fairly equal spread of good, satisfactory and poor well-being, with a third having poor well-being. 235
Facilitators and barriers to successful outcomes following reunification
Research has shown that failed reunifications are often associated with poor practice by social workers and other professionals, including:
- a lack of or poor-quality assessments of whether or not the child should return home
- passive case management
- lack of appropriate support services for children and families
- inadequate planning and preparation for return and lack of monitoring post- return. 236
Significant predictors of return stability before return included:
- the child had not been physically abused
- the child had not oscillated in and out of care
- parent's actively sought reunion, indicating motivation
- there was adequate preparation of children and parents
- there was foster carer assistance with returns.
Significant predictors of return stability after return included:
- changes to family membership since the child had lived there
- involvement of professionals in supervising the child
- adequate support during return
- no concerns about poor parenting
- the child not showing severe attachment-type difficulties. 237
Purposeful social work planning, which includes children and birth families, and allowing children to go home slowly over a longer period of time is associated with more successful returns home. 238 Children and parents also need support to overcome issues such as alcohol or drug misuse and/or mental health difficulties. 239
Wilkins and Farmer (2015) have developed an evidence-informed framework for the NSPCC to promote professional judgement in relation to children returning home from care. The key messages underpinning the framework include the need for:
- robust assessment of risk and protective factors of parental ability to care and their capacity to change
- caution when considering reunification with parents with particular risk factors such as substance misuse or previous failed return home
- considering the child's best interests and voice in decision making and planning.
- giving parents reasonable opportunity and support to change
- continuing to support, monitor and review for as long as it is needed. 240
5.3 Emotional and behavioural outcomes for children in permanent placements
As previously discussed, children who have been maltreated are at increased risk of displaying emotional and behavioural difficulties. Evidence suggests that some of these difficulties persist even after the child has been living within a nurturing loving family for some time, whatever the placement type.
Biehal and colleagues' longitudinal study of outcomes in long-term foster care and adoption found that, across the sample as a whole, 38 per cent of the children had total scores on the SDQ that indicated significant emotional and behavioural difficulties. There was no significant difference in Strengths and Difficulties Questionnaire (SDQ) scores between children in long-term foster care and those who had been adopted. However, children whose foster placements had disrupted had significantly worse SDQ scores than those in stable foster placements. 241 It is not clear from these findings whether the disruptions and severance of relationships had an impact on the child's emotional well- being or whether the emotional and behavioural difficulties caused the disruption.
For a sub-sample of 90 children who had been studied five and eight years earlier, SDQ scores generally showed little change over time. This suggests that the severity of children’s emotional and behavioural difficulties may be largely determined by pre-placement adversity and the length of children’s exposure to these adversities. 242 Key predictors of high SDQ scores were entering the current placement at the age of four or over and having a disability. 243
These findings are consistent with findings from a longitudinal study comparing outcomes associated with different long-term placements for a sample of 70 children aged 9 to 14. The sample was selected from a population of children (n=374) who were under the age of five and in care in Northern Ireland on 31 March 2000. 244 The study found that there were no significant differences in mean SDQ scores between children across five placement types: adoption; foster care; kinship foster care; residence orders; and living with birth parents. However, within each placement, there were variations with respect to the proportions scoring above the clinical threshold for Total Difficulties: 50 per cent of the children living with birth parents and 44 per cent of those in foster care scored above the clinical threshold as compared to children who were adopted, in kinship care or the subject of a residence order (28, 25 and 14 per cent respectively).
Children who live in children's homes have high levels of emotional and behavioural difficulties. Berridge and colleagues found that more than a third (38 per cent) had a statement of special educational needs, nearly two-thirds (62 per cent) had clinically significant mental health difficulties and three-quarters (74 per cent) were reported to have been violent or aggressive in the past six months. 245 Children living in children’s homes also tend to be older than children in other placements (average age 14.7 years). Children with more stable placements (i.e. placement in the home for at least a year) tend to have fewer emotional and behavioural problems than children with unstable placements. 246
Emotional and behavioural difficulties for adopted children
There is research providing evidence of the beneficial outcomes following adoption, especially with regard to helping developmental recovery following early maltreatment. As with children on other orders, some adopted children have high levels of social, emotional and behavioural difficulties. Selwyn and colleagues' study of adoption found that where such difficulties did exist, they generally began within the first few years of placement and escalated during adolescence. 247
As well as analysing administrative data, Selwyn and colleagues conducted a survey with 390 adoptive parents, and from this selected three groups of parents to explore in depth some of the factors that might explain whether the placement was going well or not. The sample comprised:
- parents whose child had left home prematurely (under the age of 18 years) ('left home' group)
- parents whose child still lived at home but where caring for them was considered very difficult ('at home' group)
- parents who had reported no or few difficulties ('going well’ group).
Children in the 'at home' and 'left home' groups displayed higher levels of social and emotional difficulties than children in the 'going well' group, indicating that many of the adopted children had a residue of difficulties that had not been overcome, making the parenting task very challenging. The children in the 'going well' group were significantly younger at the time of the adoption order than the children in the 'at home' and 'left home' groups (3.0, 4.2 and 6.2 years respectively), again highlighting the impact of age at placement on well-being and stability.
The study also found that the 'left home' and 'at home' groups show markedly elevated levels of attachment difficulties 248 (compared with the going well group), but that many of the 'going well' group also showed raised levels of attachment difficulties according to clinical cut offs. Children in all groups had received a formal diagnosis of mental health problems, although the proportions were lower for the 'going well' group compared to the other groups (29 per cent compared to 68 per cent for the 'left 'home' and 76 per cent for the 'at home' groups). Examples included:
- attachment disorders
- ADHD (attention deficit hyperactivity disorder)
- PTSD (post-traumatic stress disorder)
- FASD (foetal alcohol spectrum disorders)
- OCD (obsessive compulsive disorder)
- oppositional defiant disorder. 249
There was a rapid escalation of challenging behaviour as children reached puberty, particularly with regard to anger, aggression and control. There was also violence in the family home, leading to some parents being injured, vulnerable and frightened.
These findings illustrate the significant challenges faced by adoptive parents in parenting their children, and the need for ongoing support to ameliorate these challenges and to help their children recover from their early trauma. Despite the challenges, Selwyn and colleagues highlight the commitment and tenacity of adoptive parents in maintaining the placements. 250
Emotional and behavioural difficulties for children with SGOs
Similar difficulties were noted for children for whom special guardianship orders (SGOs) had been made, with almost a quarter (24 per cent) of the children in Wade and colleagues’ 2014 study having total scores above the SDQ clinical threshold for serious emotional and behavioural difficulties. Over a quarter of children in the survey sample were reported to have had some attachment difficulties (27 per cent) and a similar proportion (28 per cent) had shown signs of delayed development. Children who had learning disabilities were twice as likely as other children to have had difficulties in forming secure attachments or to have social, emotional and behavioural problems. As with the findings for adoption, Wade's findings highlight the parenting challenges faced by many guardians. 251
Wade and colleagues also developed a composite measure of placement progress for children and young people who were the subject of SGOs at the follow-up period. The majority of children were reported to be doing well; however, over a third were reported to have some emotional and behavioural difficulties and three in ten were not doing well in education. Children with emotional and behavioural difficulties had poorer outcomes and their challenging behaviour placed a strain on their guardians. Boys, especially those who were older at the time of the SGO, and children with learning disabilities scored more highly for these difficulties and had poorer outcomes in relation to educational progress and social skills. 252
Placement progress tended to be better:
- where children had lived with their special guardian before the order was made, and for a longer period of time
- where the bond between the guardian and child was rated as being very strong before the order was made.
The strength of the bond between the child and the guardian, alongside SDQ scores, were the strongest predictors of placement progress. As with Selwyn's study of adopted children, there was an association between the age of the child at the time of the SGO and children's overall development and well-being, with children who were older at the time of the SGO faring less well.
A Cochrane review of international evidence on outcomes of kinship foster care placements also indicates that such placements are effective and, in some cases, may be more effective than unrelated foster care. The review found that there was some evidence that children in kinship care experience better outcomes with regard to behaviour problems, psychiatric disorders, well-being and placement stability than children in unrelated foster care. 253
5.4 Stability and disruption in permanent placements
Selwyn and colleagues investigated rates of disruption for adoption ( after the adoption order was made) and compared these to the rates of disruption for SGOs and residence orders (ROs). 254 Disruption rates for all three types of order were relatively low. The orders were compared over a five-year follow-up period to offer a ‘like for like’ comparison 255. Over a five year period:
- 147 in 1,000 ROs would have disrupted
- 57 in 1,000 SGOs would have disrupted
- 7 in 1,000 adoptions would have disrupted.
Although adoption orders were the most stable, the disruptions rate rose to 3.2 per cent after children reached 12 years of age, which echoes findings discussed previously about difficulties escalating during adolescence. Data on longer-term disruption rates are not yet available for SGO and residence orders/child arrangements orders placements.
Factors associated with stability and disruption in different placements
The majority of adoption disruptions (61 per cent) occurred during the secondary school years (average age 12.7 years), after the child had been living with the family for a number of years. SGO and RO disruptions occurred irrespective of the child’s age since the making of the legal order; 75 per cent of SGO disruptions occurred within two years compared to just 14 per cent of adoption disruptions. In around two-thirds of SGO and RO disruptions, the children were under 11 years of age (compared to 14 per cent of adoptions disruptions occurring before this age). However, since data are not yet available over such a long time span for SGOs and ROs, it may be that the adolescent years pose risks for the SGO and RO placements that were continuing at the time of the study. 256
A number of factors were associated with disrupted adoptions including:
- older age at entry to care
- older age at time of adoptive placement
- more moves in foster care
- lengthier adoption processes.
Children who were four years or older when placed for adoption were 13 times more likely to experience a disruption than those who were placed as infants. 257 These findings are consistent with those of Wade et al's for special guardianship where the proportion of children returning to care averaged just over one per cent per year, but rose to an estimated rate of almost three per cent per year for children aged 9-10 when the SGO was made. 258 These findings highlight the need for timely decision making when children are unable to remain safely with their parents.
SGO and RO disruptions were less likely if the SGO or RO was made to a kinship carer. 259 These findings are consistent with other research on kinship care. For example, Hunt et al (2008) followed up a group of 113 children placed with members of their family over a number of years. They found that 72 per cent of placements were continuing or had ended having lasted as long as needed. A further 28 per cent had ended prematurely and 16 per cent were continuing but vulnerable to disruption. According to the researchers this compares to an average rate of disruption for unrelated foster care of around 43 per cent. 260
The relatively high rates of breakdown for SGOs and ROs within two years of the order being made raises questions about the assessments of carers, the making of the orders and the support provided to carers. 261 The challenges of working within a compressed timescale for completing assessments of prospective special guardians who come forward during care proceedings is a recurrent theme in recent studies on the impact of the family justice reforms on front-line practice. 262
These findings are consistent with those of Wade and colleagues who found that children who were older at the time of the SGO were at greater risk of the placement disrupting. In addition, children were more likely to experience a disruption where:
- they had been last placed with a stranger (rather than a relative) before the SGO was made
- the SGO was made to a person with whom the child had not already been living
- Research in Practice (2015) Impact of the Family Justice Reforms on Front-line Practice Phase Two: Special Guardianship Orders . London: Department for Education.
- the bond between carer and child was not rated as having been strong at the time of the SGO
- children had experienced more past placement moves. 263
Wade and colleagues noted that the strength of the pre-existing bond between the child and carer had an independent effect. Where the bond was strong, the effects of behavioural difficulties were likely to have been mitigated and risks to the placement reduced. The strength of an existing bond is therefore an important factor to consider when making decisions about a child's future, not just in the short term but through to the child reaching adulthood.
Recent research found that social work professionals have reported an increase in the number of SGOs being made to family members (and others) who do not have a strong relational bond with the child and who frequently come forward late in the care proceedings process. 264 Local authorities do not necessarily rule out extended family members who have no established relationship with the child, and in some cases such placements can be a positive outcome for a child. However, the assessment for those without an existing relationship is more complex and requires more time. Social work professionals reported that the 26-week timeframe for the PLO meant there was often insufficient time to properly assess and prepare prospective special guardians and to allow a period of settling in and testing of the placement before the order was made. 265 Making SGOs quickly, before relationships have been properly tested may carry some future risk of disruption 266, although there is no evidence to support this at present.
For children living in children’s homes, the average placement duration is similar to that of foster placements 267, although fewer last longer than a year (19 per cent compared to 32 per cent). More than a quarter of children living in children's homes have had at least five previous placements. 268
Commitment of carers
There is consistent evidence to show that adopters, special guardians, kinship carers and long-term foster carers have a commitment to the children they care for. 269 However, the routes by which they come to these roles are very different, which may have an impact on the stability of placements.
Adoptive parents often make a decision to adopt because of infertility and wanting to have their own family. They go through a rigorous assessment and preparation process and spend a period of time getting to know the child who they have been matched with before the child comes to live with them. They then have to wait a further 10 weeks before they can apply for the adoption order. Thus, adopters are generally well prepared and highly committed to providing permanent care for the child/children. 270
Evidence shows that kinship carers have a high degree of commitment to the children they care for and tend to persevere in looking after children with high levels of difficulty beyond the point at which non-kin carers would do so. 271 This is a key factor in terms of stability of the placement, but it also means that many kin carers continue to care for a child when they are under considerable strain, which can result in a poor-quality placement. Kinship carers persist in caring for their children despite having fewer financial and material resources. Farmer and Moyers (2008) found evidence of financial difficulty in 75 per cent of formal kin placements, compared to 13 per cent in non-kin placements. 272 Analysis of the 2001 census data also found that a substantial number of children (in formal and informal kin care) were living with families whose characteristics were associated with increased risk of poverty: single female carers, dependent on benefits, workless households, and higher prevalence of long-term illness or disability. 273
Special guardians are also committed to the children they care for, despite caring for challenging children in challenging circumstances. Many are grandparents who step in when their own son or daughter is not able to safely care for the child. They also go through an assessment process, but this does not generally comprise the depth and preparation that adopters go through. Because of the need to meet the timescale of the court, prospective carers may have little time to reflect on the impact on the household of looking after a child, who may have social, emotional and behavioural problems, through to adulthood. This may mean that they are less well-prepared for the challenges of looking after children (even blood relatives) who have been maltreated. Despite this, the majority of special guardians continue to care for their children under difficult circumstances, showing their high level of commitment. 274
Foster carers have a dual role as both a professional carer and a parent. When a child is placed in foster care the local authority (rather than the foster carer) has parental responsibility for the child (although foster carers have delegated authority) and any major decisions regarding the child have to be approved by the local authority. Many foster carers stick with the child or children they care for even through challenging times because of the bond and commitment they have. However, they are free to stop being a foster carer to a particular child at any point, meaning that children have, potentially, less security in foster placements. 275
Some foster carers have described the 'compassion fatigue' (numbness, suppression, and defensiveness) they feel as result of caring for children with complex needs on a daily basis. This is sometimes referred to as ‘blocked care’ in the context of fostering and adoption, a term that is used to describe parents’ emotional, physical and biological responses to children’s insecure attachment behaviours, resulting in parents no longer being able to make a healthy connection to the child. 276
Although some carers may react by withdrawing from placements in which children are emotionally distant and relationships between parents and children are under immense strain, the majority of adoptive parents and foster carers continue their commitment to support children, regardless of the circumstances. 277 Providing support to carers, whatever the placement, is key to enabling carers to therapeutically parent children who have been maltreated.
Information on children's needs prior to placement is also crucial. However, there is evidence that information sharing, and the quality of the information, is sometimes poor at the matching stage for adoption, especially with regard to children’s emotional and behavioural difficulties. 278 Lack of (or poor-quality) information has also been noted by special guardians when they have stepped in to care for the child of a family member (or close friend). 279 Poor information means that specific needs can be either minimised or not identified. If carers are not prepared for difficulties then the placement is vulnerable to disruption.
Children's sense of belonging and permanence
Another important element of permanence and stability is children's perceptions of 'belonging to' their family. Biehal and colleagues study of long-term foster care and adoption found that the majority of adopted children identified with and felt emotionally secure in their adoptive families and assumed that they would stay with their adoptive families long term. 280 This view was also reflected in Selwyn and colleagues' study of adoption. 281
Most of the children settled in long-term foster care also felt a sense of belonging and viewed their foster carers as parental figures. Some of the children had been placed with their foster carers since infancy and had no direct contact with their birth family. These long-term placements were quasi-adoptive in nature and these children also assumed they would stay with their foster family in the long term. However, some children in stable foster care had more ambivalent feelings towards their birth family and foster carers and experienced conflicts of loyalty as a result. 282
Wade and colleagues’ study similarly found that most special guardians thought their children had integrated well into the family. The granting of the order had enabled the guardians to feel more secure in their parenting role and that they could provide a safe and stable placement. Several special guardians also reported that the child felt like one of their own. Family integration tended to be higher where guardians felt well prepared and supported by their own immediate families. Frequent contact with birth mothers, however, could result in mixed experiences. Although frequent contact was welcomed and rated (where it was positive) as beneficial for the child, family integration could be lower in these cases as some children experienced divided loyalties and thought they might be able to return to their mothers. 283
Kinship care is also often a positive permanency option as it enhances children’s sense of belonging (through continuity of family identity), which is a key factor in terms of placement stability. The findings from Wade et al's study are consistent with the evidence on informal kinship arrangements. One study found that most of the children living in kinship care had a strong bond to their carer, with 97 per cent of the children reporting that living with their kinship carer was a good thing. However, more than a third of the children reported that there was a stigma attached to living in kinship care and said that there had been hurtful remarks directed towards them. 284
5.5 Educational progress for children on different orders
There is evidence that the educational achievement of looked after children falls below that of non-looked after children. In 2015, for example, 52 per cent of looked after children achieved level 4 or above at key stage 2 (KS2) for reading, writing and maths, compared to 80 per cent of non-looked after children. Similarly, 16 per cent of looked after children achieved grades A*-C in GCSE English and maths compared to 55 per cent of non-looked after children. 285 However, there are a number of potential reasons to explain the lower educational achievement of looked after children, which may not be as a result of being in care:
- their pre-care experiences, particularly where children have experienced abuse and neglect
- the higher prevalence of learning and behavioural problems amongst this group of children
- placement instability and/or educational instability (school moves) experienced by some looked after children. 286
A recent systematic review of evidence found that the strength of the relationship between being in care and educational outcomes is reduced when other individual characteristics such as gender, ethnicity and special educational needs, which are known to be linked to attainment, are taken into consideration. The review also suggested that lower educational achievement is partly explained by pre-care experiences such as abuse and neglect and that the difficulties experienced by these children and young people often persist after they have been removed from an adverse environment and placed with alternative carers. 287
These findings are consistent with those from a recent study that linked data from the National Pupil Database (NPD) and the data on Children Looked After in England (SSDA903) to explore the relationship between educational outcomes and young people's care histories and individual characteristics. 288 The sample included:
- children looked after long term, early entry: children who were in care for 12 months or more continuously at the end of key stage 4 (KS4: age 15-16) and who were also in care at the end of key stage 2 (KS2: age 10-11)
- children looked after long term, late entry: children who were in care for 12 months or more continuously at the end of KS4 but not in care at the end of KS2
- children looked after, short term: a shorter-stay group of children who were in care for less than 12 months at the end of KS4
- children in need at the end of KS4 but who were not in care
- comparison group: children who were not in care and not in need at the end of KS4.
As would be expected, the comparison group out-performed all other groups on measures of attainment at KS4, followed by the longer-stay looked after children (early and late entry). The shorter-stay group did the least well. Although some looked after children performed similarly to the non-looked after children, a sizeable minority had very low scores, thereby reducing the average scores.
Young people in care with lower prior attainment often made good progress, indicating the benefit to them of being in care. The long-term looked after children early-entry group made greater progress over time than the other groups of children in care or in need. The educational performance of the long-term late-entry group worsened relative to the early- entry group and the comparison group, but not as much as the children in need group and noticeably less than the children looked after short-term group.
These findings suggest that foster care can provide a protective factor with early admission to care associated with better educational outcomes. Although foster care may benefit late admissions, it does not fully reverse the adverse impact of the children's previous experiences. The evidence suggests that the earlier children enter care (when it is in their best interests to do so), the better their educational progress, provided that they do not experience many short-stay care periods.
One of the characteristics of children who are looked after is the high proportion who have special educational needs (SEN): 70 per cent of the long-term looked after children and children in need groups had a SEN statement or school action plan, compared to 16 per cent of children in the comparison group. The primary type of SEN was for behavioural and emotional difficulties. 289
A number of factors predicted poorer KS4 scores for the long-term looked after children when performance at KS2 was controlled for, including:
- being male
- having a special education needs statement
- entering care primarily due to disability
- having a high average SDQ score
- having more changes of placement
- changing schools in year 10 or 11
- being in a non-mainstream school at KS4
- missing school due to fixed-term exclusions. 290
5.6 Support needs of children and families
The findings that have been presented throughout this report point to the need for ongoing and, in some cases, intensive support for children who have been maltreated and their permanent carers, regardless of the placement type. Children's experiences of abuse and neglect leave them at risk of having emotional, behavioural and mental health problems, which can continue long after they have been removed from the adverse environment and placed with nurturing carers. Support also needs to be available for birth parents to address problems that result in their children being removed because of significant harm or the risk of significant harm.
Management of and support for the problems that maltreated children can face is critical to building positive outcomes for children and young people. The mental health needs of children should, therefore, be treated with the same level of concern as their physical health needs, and service availability should be provided according to children’s needs and not legal status and/or placement type. 291 There is also a need to support children who are permanently removed from birth parents in addressing issues around separation, attachment, loss and identity. 292
Whatever the placement type, carers also need as much information as possible on the needs of the children they are proposing to care for prior to the order being made. Prospective adopters go through a rigorous preparation and assessment process, which generally takes around six months to complete. Research suggests that group preparation is generally well received and that people learn a lot about the experiences and needs of children who are placed for adoption. 293 Similar preparation and training is not currently a requirement for carers who become special guardians or kinship carers, despite children who are the subject of the order having similar backgrounds and needs.
There is an equally important need to provide support to children and families on the 'edge of care' to address the issues that impact on the needs of children, so that they are able to remain safely at home where it is in the best interests of the child. 294
Assessing the immediate and ongoing support needs of any carer, regardless of placement type, is therefore an essential part of the decision making process. Carers and their support needs are not homogenous and will also vary over time. Carers may need a variety of support, which might include financial help; advice, information and advocacy; training; peer support and mentoring; specific support regarding contact; and therapeutic services for children and for their carers. 295
Conclusion
This report has summarised evidence related to:
- the impact of abuse and neglect on outcomes for children
- the strengths and weaknesses of different placements.
As has been shown, this is a complex area and research is ever evolving and, in some areas, is contested. The needs, vulnerabilities, protective factors and contextual circumstances of the individual child is paramount in any recommendations from the local authority and decisions from the court. Professional judgement based on analytical holistic assessment, the voice of the child and those close to them, and legal frameworks are all essential components of decision making. Research can guide assessment and decision making and there are some over-arching messages from research offered in conclusion.
Key messages
- Abuse and neglect have adverse impacts for most children, affecting in particular emotional, behavioural and mental well-being. These impacts appear to be cumulative and vary depending on a number of factors, including severity of the maltreatment, its duration, the age of the child and the individual susceptibilities and resiliencies of the child.
- Neglect is the most prevalent form of maltreatment. However, it can be difficult for professionals to identify and to provide evidence on whether the threshold for social work intervention and/or court action has been reached. Decision makers need to be particularly alert to this form of maltreatment, and to have a good understanding of the contextual factors that increase the risk of neglect occurring.
- It is important to identify and understand the individual, community and societal factors that interact either to increase or decrease the risk and impact of maltreatment. A holistic assessment is key to this.
- Providing earlier, effective and holistic support to parents, whilst keeping the child's welfare in mind, can reduce the risk of maltreatment.
- Where children are no longer able to remain safely with their parents, timely decisions about permanence are needed because the age of the child at entry to care has been consistently found to be associated with the stability of placements and children's well-being. The need for timely decision making needs to be balanced with robust and analytical assessment to ensure that children's welfare remains at the centre of any decisions.
- Children and young people enter care for a variety of reasons and there is no single placement that will suit all children. The 'right' placement for individual children depends on a variety of factors and decision makers need to weigh up the
- pros and cons of the different permanence options to determine which placement will best meet children's needs through the whole of their childhood and beyond.
- Children who have been maltreated generally have better outcomes with regard to stability and well-being if they are placed in alternative care that can meet their needs, particularly if the issues relating to maltreatment have not been addressed.
- Positive changes to the caregiving environment, in the form of providing nurturing and consistent care, can help children to recover from their experiences of maltreatment. However, some of the social, emotional and behavioural difficulties persist even after children move to a nurturing and stable environment.
- Adoption, special guardianship, kinship care, residence orders/child arrangements orders and long-term foster care can all offer permanence options for children who are not able to be reunified with their parents. However, they are not legally equivalent and the permanence they offer differs in certain key respects. This needs to be taken into consideration when making decisions about the child's future in both the long and short term.
- Adoption has a lower rate of disruption compared to special guardianship orders and child arrangements orders/residence orders. Adoption disruptions tend not to occur until the adolescent years, after children have been living with adoptive parents for a number of years. In contrast, SGOs and residence orders tend to disrupt within two years of the order being made, although evidence about the disruption of these placements during adolescence is currently not available.
- Information, advice and support for carers of children in permanent placements are crucial. Such support can help carers understand the impact of maltreatment on children's behaviour, and so to assist them with developmental recovery. Carers will have different support needs depending on their individual circumstances; these will vary over time and might include any combination of financial, practical and emotional support.
- Children and young people may also need specialist therapeutic support to help them recover from adverse impacts of maltreatment and to make sense of their experiences.
- Effective support also needs to be available for birth parents to address problems that result in their children being removed because of significant harm or the risk of significant harm.
- Relationships matter a great deal. Relational connectedness and identity are important considerations in decision making, particularly in relation to placing children with their siblings and in making arrangements for contact with birth relatives. There are a number of benefits both to placing siblings together and to maintaining contact with birth families; however, in some cases, it may not be in the best interests of children to be placed with siblings or to have contact with birth parents.
- It is critically important to ascertain the views and wishes of children when making decisions about their future. Children need to feel informed and listened to by those who make decisions about their lives. Every professional involved in the decision making process has a role to play in this.
Areas where further research would be useful
Based on the evidence presented in this review, there are a number of areas where further research would be beneficial.
- Small-scale qualitative studies have provided some important findings on the impact of the family justice reforms on local authority practice and decision making. To date there has been no research to investigate the impact of the reforms and recent case law on judicial decision making and the long-term outcomes for children of decisions made by the court. 296
- Evidence on the use of special guardianship and outcomes for children who are the subject of a special guardianship order (SGO) derives primarily from the work of Wade and colleagues (2014) using administrative data for looked after and non- looked after children in the period 2006-12. Since this study was completed, there has been an increase in the number of SGOs being made, accompanied by an increase in younger children becoming the subject of SGOs. Concerns have also been raised by social work professionals about SGOs being made in compressed timescales when prospective special guardians come forward during care proceedings and/or where there is no existing relationship between the child and the guardian. Further research is needed on the use of SGOs since the introduction of the revised PLO and the longer-term outcomes for children.
- Long term foster care can be a positive permanence option for many children. However, there is limited data and research on outcomes for children who are placed in long-term foster care. Further research on this would enable comparisons to be made with other permanent placements.
- Decisions regarding the placement of siblings can be very complex. At the present time, it is not possible to determine from administrative data where siblings have been involved in the same set of care proceedings, and the placement outcomes for these children. Further research would be useful on sibling placement decisions and the longer-term outcomes for children placed together or apart. 297
- There is also limited data and research on looked after children who have disabilities and the placement and long-term outcomes for these children.
- Children who have been maltreated often have social, emotional, behavioural and mental health difficulties. Further research on the nature of these difficulties and therapeutic approaches that can help to mitigate them would be helpful.
- There are also gaps in the evidence base around the pathways into and out of care for adolescents and what works in securing the best outcomes for young people who enter care during adolescence.
- More research around the role that fathers/partners play, not only in relation to being a risk factor for maltreatment, but also in being a protective factor in reducing the risk of maltreatment and mitigating the impact of maltreatment that has already occurred would be very useful.
Appendix 1: Members of the steering group
- Tracey Budd (Nuffield Foundation)
- Ross Campbell (Department for Education)
- David Duffett (Department for Education)
- District Judge Andrew Greensmith
- Elizabeth Isaacs QC
- Maura Lantrua (Department for Education)
- Helen Johnston (Cafcass)
- Mathew Pinnell (Cafcass Cymru)
- Her Honour Judge Jane Probyn
- Nicky Rayner (ADCS)
- John Simmonds (Coram BAAF)
- Reema Subhan (Ministry of Justice)
- Amy Summerfield (Ministry of Justice)
- James Thomas (ADCS)
- Eleanor Wilkes (Department for Education)
- Kevin Woods (Department for Education)
Appendix 2: Definitions of different types of maltreatment 298
|
|
Description |
|
Physical abuse |
A form of abuse which may involve hitting, shaking, throwing, poisoning, burning or scalding, drowning, suffocating or otherwise causing physical harm to a child. Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child. |
|
Sexual abuse |
Forcing or enticing a child or young person to take part in sexual activities, not necessarily involving a high level of violence, whether or not the child is aware of what is happening. The activities may involve physical contact, including assault by penetration (for example, rape or oral sex) or non- penetrative acts such as masturbation, kissing, rubbing and touching outside of clothing. They may also include non-contact activities, such as involving children in looking at, or in the production of, sexual images, watching sexual activities, encouraging children to behave in sexually inappropriate ways, or grooming a child in preparation for abuse (including via the internet). |
|
Emotional abuse |
The persistent emotional maltreatment of a child such as to cause severe and persistent adverse effects on the child’s emotional development. It may involve conveying to a child that they are worthless or unloved, inadequate, or valued only insofar as they meet the needs of another person. It may include not giving the child opportunities to express their views, deliberately silencing them or ‘making fun’ of what they say or how they communicate. It may feature age or developmentally inappropriate expectations being imposed on children. These may include interactions that are beyond a child’s developmental capability, as well as overprotection and limitation of exploration and learning, or preventing the child participating in normal social interaction. It may involve seeing or hearing the ill-treatment of another. It may involve serious bullying (including cyber bullying), causing children frequently to feel frightened or in danger, or the exploitation or corruption of children. Some level of emotional abuse is involved in all types of maltreatment of a child, though it may occur alone. |
|
Neglect |
The persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse. Once a child is born, neglect may involve a parent or carer failing to:
It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs. |
Appendix 3: Types of neglect 299
|
Neglect type |
Features associated with type of neglect |
|---|---|
|
Educational neglect |
Where a parent/carer fails to provide a stimulating environment or show an interest in the child’s education at school. They may fail to respond to any special needs and fail to comply with state requirements about school attendance. |
|
Emotional neglect |
Where a parent/carer is unresponsive to a child’s basic emotional needs. They may fail to interact or provide affection, undermining a child’s self-esteem and sense of identity. (Most experts distinguish between emotional neglect and emotional abuse by intention; emotional abuse is intentionally inflicted, emotional neglect is an omission of care.) |
|
Medical neglect |
Where a parent/carer minimises or denies a child’s illness or health needs and/or fails to seek appropriate medical attention or administer medication and treatment. |
|
Nutritional neglect |
Where a child does not receive adequate calories or nutritional intake for normal growth (also sometimes called ‘failure to thrive’). At its most extreme, nutritional neglect can take the form of malnutrition. |
|
Physical neglect |
Where a parent/carer does not provide appropriate clothing, food, cleanliness and/or living conditions. |
|
Supervisory neglect |
Where a parent/carer fails to provide an adequate level of supervision and guidance to ensure a child’s safety and protection from harm. For example, a child may be left alone or with inappropriate carers, or appropriate boundaries about behaviours (for example, under-age sex or alcohol use) may not be applied. |
Appendix 4: Summary of selected UK research studies
[Editor's note: see PDF for full table of data]
Footnotes
-
For example: An Action Plan for Adoption - Tackling delay (2012), Special Guardianship Review: Report on findings (2015), Children's Social Care Reform: A vision for change (2016), Adoption: A vision for change (2016)
-
Adoption: A new approach (2000)
-
Children and Families Act (2014)
-
Department for Education (2016) Putting Children First: Delivering our vision for excellent children's social care
-
Family Court Statistics Quarterly, England and Wales. January to March 2016
-
Beckett, C., Dickens, J. and Bailey, S. (2016) Outcomes for children of shorter court decision-making processes: A follow-up study of the Tri-borough care proceedings pilot. University of East Anglia.
-
Data supplied to Research in Practice by the Ministry of Justice.
-
Cafcass: Public Law Data - Care and private law demand statistics
-
Children looked after in England (including adoption) year ending 31 March 2016 SFR41/2016
-
ibid.
-
Supreme Court and Court of Appeal judgements (Re B and Re B-S) emphasised the significance of an order for adoption as ‘a very extreme thing, a last resort’ to be made ‘only in exceptional circumstances and where motivated by overriding requirements pertaining to the child's welfare, in short, where nothing else will do’ (Re B para. 74 and 215). Re B-S cited Re B and emphasised the high standard of evidence and reasoning required by the court in non-consensual adoption cases and the need to present an analysis of the arguments for and against all realistic options for the child. Following concerns that local authorities had misinterpreted the judgements in Re B and Re B-S, the National Adoption Leadership Board published a 'Myth-Buster' guide (National Adoption Leadership Board, 2014). The interpretation of Re B-S was also addressed by the President of the Family Division in a judgement handed down in December 2014 (Re R) which re-emphasised that there was no change in the law and that local authorities should not shy away from seeking care orders with a plan for adoption when it is in the best interests of the child.
-
Children looked after in England (including adoption) year ending 31 March 2016 SFR41/2016
-
Woolgar, M. (2013) 'The practical implications of the emerging findings in the neurobiology of maltreatment for looked after and adopted children: Recognising the diversity of outcomes'. Adoption & Fostering, 37 (3) 237-252.
-
Although they are used to evaluate the effectiveness of some interventions.
-
Woolgar, M. (2013) op. cit.
Wastell, D. and White, S. (2012) 'Blinded by neuroscience: Social policy, the family and the infant brain'. Families, Relationships and Society, 1 (3) 397–414.
-
For example: The Munro Review of Child Protection: Final Report
-
ibid.
-
Courts and Tribunals Judiciary: Independence
-
HM Government (2015) Working together to safeguard children. A guide to inter-agency working to safeguard and promote the welfare of children. [No longer online]
-
ibid.
-
Butchart, A., Harvey, A., Mian, M. and Kahane, T. (2006) Preventing Child Maltreatment: A guide to taking action and generating evidence. Geneva: World Health Organization. (p.9)
-
Sidebotham, P., Brandon, M., Bailey, S. and Belderson, P., et al (2016) Pathways to Harm, Pathways to Protection: A triennial analysis of serious case reviews 2011 to 2014. London: Department for Education.
-
Cleaver, H., Unell, I. and Aldgate, J. (2011) Children's Needs – Parenting Capacity. Child abuse: Parental mental illness, learning disability, substance misuse and domestic violence. London: The Stationery Office.
Brandon, M., Bailey, S. and Belderson, P. (2010) Building on the Learning from Serious Case Reviews: A two-year analysis of child protection database notifications 2007-2009. London: Department for Education.
Sidebotham, P. et al (2016) op. cit.
Bellis, M., Ashton, K., Hughes, K., Ford. K. et al (2015) Adverse Childhood Experiences and their impact on health-harming behaviours in the Welsh adult population. Public Health Wales NHS Trust.
-
Cleaver, H. et al (2011) op. cit.
Stanley, N. (2011) Children Experiencing Domestic Violence: A research review. Dartington: Research in Practice.
-
Children Act 1989, s.31(9)
-
Cleaver, H. et al (2011); Stanley, N. (2011) op. cit.
-
Women's Aid (2015) Change that Lasts: Transforming responses to domestic violence and abuse. (p.1)
-
Horwath, J. (2016) 'Making a difference to the neglected child's lived experience'. In Gardner R. (ed) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
-
Rushton, A. and Dance, C. (2003) 'Preferentially rejected children and their development in permanent family placements'. Child and Family Social Work, 8 (4) 257-267.
-
Bywaters, P., Bunting, L., Davidson, G., Hanratty, J. et al (2016) The Relationship between Poverty, Child Abuse and Neglect: An evidence review. York: Joseph Rowntree Foundation.
-
ibid.
-
Bywaters, P., Brady, G., Sparks, T. and Bos, E. (2014) 'Inequalities in child welfare intervention rates: The intersection of deprivation and identity'. Child & Family Social Work, doi. 10.1111/cfs.12161. Accessed 17/11/16.
-
Sidebotham, P. and Heron, J. (2006) 'Child maltreatment in the "children of the nineties": A cohort study of risk factors'. Child Abuse & Neglect, 30 (5) 497-522.
-
Brown, R. and Ward, H. (2016) Eight-year-olds Identified in Infancy as at Risk of Harm: Report of a prospective longitudinal study. London: Department for Education.
-
Coleman, J. (2014) Understanding Adolescence. Dartington: Research in Practice
Cleaver, H., Unell, I. and Aldgate, J. (2011) Children's Needs – Parenting Capacity. Child abuse: Parental mental illness, learning disability, substance misuse and domestic violence. London: The Stationery Office.
-
Platt, D. and Turney, D. (2012) 'Editorial: Parental engagement with services when children may be at risk'. Child & Family Social Work, 17 (2) 115-117.
-
Featherstone, B., White, S. and Morris, K. (2016) Re-imagining Child Protection. Towards humane social work with families. Policy Press.
For practice innovation see for instance the decrease in looked after children numbers attributed to the work of Leeds City Council using family group conferencing.
-
White, O., Hindley, N. and Jones, D. (2015) ‘Risk factors for child maltreatment recurrence: An updated systematic review’. Medicine, Science and the Law, 55 (4) 259-277.
Centers for Disease Control and Prevention: ‘Child Abuse and Neglect: Risk and protective factors’ [No longer online]
-
Early Intervention Foundation: ‘How do we know early intervention works?’
Davies, C. and Ward, H. (2012) Safeguarding Children Across Services: Messages from Research on Identifying and Responding to Child maltreatment. London: Jessica Kingsley Publishers.
-
Davies, C. and Ward, H. (2012) op. cit.
-
Bentley, H., O’Hagan, O., Raff, A. and Bhatti, I. (2016) How Safe are Our Children? The mostcomprehensive overview of child protection in the UK 2016. London: NSPCC.
-
See: Davies, C. and Ward, H. (2012) op. cit.
Allnock, D. (2016) Exploring the Relationship between Neglect and Adult-perpetrated Intrafamilial Child Sexual Abuse: Evidence Scope 2. Dartington: Research in Practice.
Allnock, D. 'Child Neglect. The research landscape'. In Gardner, R. (2016) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers
-
2,160 parents or guardians of children and young people under 11 years of age (under-11s); 2,275 young people between the ages of 11 and 17 (11-17s), with additional information provided by their parents or guardians; 1,761 young adults between the ages of 18 and 24 (18-24s).
-
Radford, L., Corral, S., Bradley, C., Fisher, H. et al (2011) Child Abuse and Neglect in the UK Today. London: NSPCC.
-
ibid. (p.23): Severe maltreatment was defined on the basis of the type of maltreatment, its frequency, whether there were multiple forms, an injury, whether a weapon had been used, if it was defined by the victim as being abusive or would fall into a more severe category of abuse under the criminal law.
-
ibid.
-
ACEs are defined as stressful experiences occurring during childhood that directly harm a child or affect the environment in which they live.
-
Bellis, M., Ashton, K., Hughes, K., Ford. K. et al (2015) Adverse Childhood Experiences and their impact on health-harming behaviours in the Welsh adult population. Public Health Wales NHS Trust.
-
If the local authority identifies there is reasonable cause to suspect the child is suffering, or is likely to suffer significant harm, it will carry out an assessment under section 47 of the Children Act 1989 to determine if it needs to take steps to safeguard and promote the welfare of the child.
-
Department for Education (2016) Characteristics of Children in Need: 2015 to 2016: SFR52/2016
-
Schumacher, J., Smith-Slep, A., and Heyman, R. (2001). ‘Risk factors for child neglect’. Aggression and Violent Behavior, 6 (2-3) 231-254.
Rees, G., Stein, M., Hicks, L. and Gorin, S. (2011) Adolescent Neglect. Research, policy and practice. Jessica Kingsley Publishers.
-
Sidebotham, P., Brandon, M., Bailey, S. and Belderson, P., et al (2016) Pathways to Harm, Pathways to Protection: A triennial analysis of serious case reviews 2011 to 2014. London: Department for Education.
-
Tanner, K. and Turney, D. (2003) 'What do we know about child neglect? A critical review of the literature and its application to social work practice'. Child and Family Social Work, 8 (1) 25-34.
Gardner, R. (ed.) (2016) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
-
Brandon, M., Bailey, S., Belderson, P. and Larsson, B. (2013) Neglect and Serious Case Reviews. A report from the University of East Anglia commissioned by NSPCC. London: NSPCC.
-
HM Government (2015) Working Together to Safeguard children. A guide to inter-agency working tosafeguard and promote the welfare of children. [No longer online]
-
Brandon, M. et al (2013) op. cit.
-
Brandon, M., Glaser, D., Maguire, S., McCrory, E. et al (2014) Missed Opportunities: Indicators of neglect – what is ignored, why, and what can be done? London: Department for Education.
-
ibid.
-
Baynes, P. and Holland, S. (2012) ‘Social work with violent men: A child protection file study in an English local authority.’ Child Abuse Review 21 (1) 53-65.
-
Children with disabilities was included as a specific theme in this review following discussions with the Department for Education; other groups of children may also have a heightened risk of being maltreated but are not explored within this review.
-
Stalker, K. and McArthur, K. (2012) 'Child abuse, child protection and disabled children: A review of recent research'. Child Abuse Review, 21 (1) 24-40.
Miller, D. and Brown, J. (2014) 'We have the right to be safe'. Protecting disabled children from abuse. London: NSPCC.
-
Stalker, K. and McArthur, K. (2012) op. cit.
-
Bywaters, P., Brady, G., Sparks, T. and Bos, E. (2014) 'Inequalities in child welfare intervention rates: the intersection of deprivation and identity'. Child & Family Social Work, doi. 10.1111/cfs.12161.
-
Brandon, M., Sidebotham, P., Bailey, S., Belderson, P. et al (2012) New Learning from Serious Case Reviews: A two year report for 2009-2011. London: Department for Education.
-
Sidebotham, P. et al (2016) op. cit.
-
Murray, M. and Osborne, C. (2009) Safeguarding Disabled Children. Practice guidance. London: DCSF.
Miller, D. and Brown, J. (2014) op. cit.
-
Sidebotham, P. et al (2016) op. cit.
Contact a Family (2012): Forgotten Families. The impact of isolation on families with disabled children across the UK. London: Contact a Family.
-
Davies, C. and Ward, H. (2012) Safeguarding Children Across Services: Messages from research on identifying and responding to child maltreatment. London: Jessica Kingsley Publishers.
-
Hildyard, K. and Wolfe, D. (2002) 'Child neglect: developmental issues and outcomes'. Child Abuse & Neglect, 26 679–695.
Gardner, R. (2008) Developing an Effective Response to Neglect and Emotional Harm to Children. University of East Anglia and NSPCC.
Schrader-McMillan, A. and Glaser, D. (2014) Emotional Abuse and Neglect: Identifying and responding in practice with families. Frontline briefing. Dartington: Research in Practice.
Cleaver, H., Unell, I. and Aldgate, J. (2011) Children's Needs – Parenting Capacity. Child abuse: Parental mental illness, learning disability, substance misuse and domestic violence. London: The Stationery Office.
-
Woolgar, M. (2013) ‘The practical implications of the emerging findings in the neurobiology of maltreatment for looked after and adopted children: Recognising the diversity of outcomes’. Adoption & Fostering, 37 (3) 237-252 (p.239)
-
Allnock, D. (2016) Exploring the Relationship between Neglect and Adult-perpetrated Intrafamilial Child Sexual Abuse: Evidence Scope 2. Dartington: Research in Practice.
Tanner, K. and Turney, D. (2003) 'What do we know about child neglect? A critical review of the literature and its application to social work practice'. Child and Family Social Work, 8 (1) 25-34.
Hildyard, K. and Wolfe, D. (2002) op. cit.
-
Brandon, M., Glaser, D., Maguire, S., McCrory, E. et al (2014) Missed Opportunities: indicators of neglect – what is ignored, why, and what can be done? London: Department for Education.
-
Tanner, K. and Turney, D. (2003) op. cit.
-
Hanson, E. (2016) Exploring the Relationship between Neglect and Child Sexual Exploitation: Evidence Scope 1. Dartington: Research in Practice.
-
Sidebotham, P., Brandon, M., Bailey, S. and Belderson, P., et al (2016) Pathways to Harm, Pathways to Protection: A triennial analysis of serious case reviews 2011 to 2014. London: Department for Education.
-
See: Bowlby, J. (1980) The Making and Breaking of Affectional Bonds. London: Tavistock; Ainsworth, M., Biehar, M. and Waters, E. (1978) Patterns of Attachment: A psychological study of the strange situation. New Jersey: Lawrence Erlbaum Associates.
-
Bolen R (2000) 'Validity of Attachment Theory'. Trauma, Violence and Abuse. 1 (2) 128-153.
-
National Collaborating Centre for Mental Health (2015) Children's Attachment. Attachment in children and young people who are adopted from care, in care or at high risk of going into care. NICE Guideline 26.
Howe, D. (2009) 'The impact of histories of abuse and neglect on children in placement'. In Schofield, G. and Simmonds, J. (eds) The Child Placement Handbook. Research, policy and practice. London: BAAF.
Schofield, G. and Beek, M. (2006) Attachment Handbook for Foster Care and Adoption. London: BAAF.
-
Moretti, M. and Peled, M. (2004) 'Adolescent-parent attachment: Bonds that support healthy development'. Paediatrics & Child Health, 9 (8) 551-555.
-
Dayton, C., Levendosky, A., Davidson, W. and Bogat, G. (2010) ‘The child as held in the mind of the mother: The influence of prenatal maternal representations on parenting behaviours.’ Infant Mental Health Journal, 31 (2) 220-241.
-
Shemmings, D. (2011) Attachment in Children and Young People. Frontline briefing. Dartington: Research in Practice.
-
National Collaborating Centre for Mental Health (2015) op. cit.
-
Benoit, D. (2004) 'Infant-parent attachment: Definition, types, antecedents, measurement and outcome'. Paediatrics & Child Health, 9 (8), 541–545.
-
National Collaborating Centre for Mental Health (2015) op. cit.
-
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders (DSM-5)
-
Woolgar, M. and Baldock, E. (2015). 'Attachment disorders versus more common problems in looked after and adopted children: Comparing community and expert assessments'. Child and Adolescent Mental Health, 20 (1) 34-40.
-
ibid.
-
Woolgar, M. (2013) ‘The practical implications of the emerging findings in the neurobiology of maltreatment for looked after and adopted children: Recognising the diversity of outcomes’. Adoption & Fostering, 37 (3) 237-252.
-
Barlow, J. (2016) 'The effects of emotional neglect during the first two years of life'. In Gardner R. (ed) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
-
Sroufe, A. (2005) 'Attachment and development: A prospective, longitudinal study from birth to adulthood'. Attachment & Human Development, 7 (4) 349-367.
-
Thompson, R. and Raikes, H. (2003) 'Toward the next quarter-century: Conceptual and methodological challenges for attachment theory'. Development and Psychopathology, 15 (3) 691-718.
-
Barlow, J. (2016) op. cit.
-
Woolgar (2013) op. cit. (p.249)
-
Belsky, J. and de Haan, M. (2010) 'Annual research review: Parenting and children’s brain development: the end of the beginning'. Journal of Child Psychology and Psychiatry, 52 (4) 409-428. doi:10.1111/j.1469- 7610.2010.02281.x
-
ibid.
Jaffee, S. and Christian, C. (2014) ‘The biological embedding of child abuse and neglect’. Social Policy Report, Vol. 28 No. 1.
National Scientific Council on the Developing Child (2012) The Science of Neglect: The persistent absenceof responsive care disrupts the developing brain. Working Paper 12.
-
McCrory, E. and Viding, E. (2015) 'The theory of latent vulnerability: Reconceptualizing the link between childhood maltreatment and psychiatric disorder'. Development and Psychopathology, 27, 493-505.
-
Woolgar, M. (2013) op.cit.
-
Department of Education: Children looked after in England (including adoption) year ending 31 March 2016. SFR41/2016
-
See for example: Biehal, N., Ellison, S., Baker, C. and Sinclair, I. (2010) Belonging and Permanence: Outcomes in long-term foster care and adoption. London: BAAF.
Wade, J., Biehal, N., Farrelly, N. and Sinclair, I. (2011) Caring for Abused and Neglected Children: Making the right decisions for reunification or long-term care. London: Jessica Kingsley Publishers.
Selwyn, J., Wijedasa, D. and Meakings, S. (2014)Beyond the Adoption Order: Challenges, interventions and adoption disruption. London: Department for Education.
Meltzer, H., Gatward, R., Corbin, T., Goodman, R. and Ford, T. (2003) The Mental Health of Young People Looked After by Local Authorities in England. London: The Stationery Office.
-
The SDQ comprises measures in relation to: emotional symptoms, conduct (behaviour) problems, hyperactivity, peer problems, and pro-social behaviours. The cut-off points of the SDQ have been calculated so that only 10-15 per cent of children in the general population would be expected to have scores over the clinical threshold for severe emotional and behavioural problems. An abnormal total score is 17 or above.
-
Ford, T., Vostanis, P., Meltzer, H. and Goodman, R (2007) ' Psychiatric disorder among British children looked after by local authorities: Comparison with children living in private households.' British Journal of Psychiatry, 190 (3) 19-325.
-
Biehal, N., et al (2010) op. cit.
-
Sempik, J., Ward, H. and Darker, I. (2008) 'Emotional and behavioural difficulties of children and young people at entry into care'. Clinical Child Psychology and Psychiatry, 13 (2) 221-233.
-
Munro, E. and Hardy, A. (date unknown) Placement Stability: A review of the literature. Loughborough University. Downloaded 23/01/17.
-
Rubin, D., O’Reilly, A., Luan, X. and Localio, A. (2007). 'The impact of placement stability on behavioural well-being for children in foster care'. Pediatrics, 119 (2), 336-344.
-
Ford, T. et al (2007) op. cit.
Norman R., Byambaa M, De R., Butchart A., Scott, J. et al (2012) 'The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis'. PLoS Med9 (11): e1001349. doi:10.1371/journal.pmed.1001349.
McCrory, E. and Viding, E. (2015) 'The theory of latent vulnerability: Reconceptualizing the link between childhood maltreatment and psychiatric disorder'. Development and Psychopathology, 27 (2) 493-505.
-
Norman, R. et al (2012) op. cit.
-
Meltzer, H. et al (2003) op.cit.
-
Unknown.
-
Ford, T. et al (2007) op. cit.
-
Table taken from: Bazalgette, L., Rahilly, T. and Trevelyan, G. (2015) Achieving Emotional Wellbeing forLooked After Children. A whole system approach. London: NSPCC. (p.12)
-
See Chapter 6 of Key Data on Adolescence 2015 (Association for Young People’s Health)
-
McAllister, J. and Lee, W. (2016) 'Child neglect and the development of communication'. In Gardner, R (ed) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
-
Mills, C. (2007) Problems at Home, Problems at School. The effects of maltreatment in the home and children's functioning at school: an overview of recent research. London: NSPCC.
-
Biehal, N., Ellison, S., Baker, C. and Sincliar, I. (2010) Belonging and Permanence: Outcomes in long- term foster care and adoption. London: BAAF.
-
Mills. C. (2007) op. cit.
-
ibid.
-
Sebba, J., Berridge, D., Luke, N., Fletcher, J. et al (2015) The Educational Progress of Looked After Children in England: Linking care and educational data. Oxford: Rees Centre.
-
Cleaver, H., Unell, I. and Aldgate, J. (2011) Children's Needs – Parenting Capacity. Child abuse: Parental mental illness, learning disability, substance misuse and domestic violence. London: The Stationery Office.
-
Ward, H., Brown, R. and Maskell-Graham, D. (2012) Young Children Suffering, or Likely to Suffer, Significant Harm: Experiences on entering education. London: Department for Education.
Sidebotham, P., Brandon, M., Bailey, S. and Belderson, P., et al (2016)Pathways to Harm, Pathways to Protection: A triennial analysis of serious case reviews 2011 to 2014. London: Department for Education.
-
British Medical Association (June 2007, updated February 2016) Alcohol and Pregnancy: Preventing and managing fetal alcohol spectrum disorders. London: BMA.
-
ibid.
-
Cleaver, H. et al (2011) op. cit.
-
Stanley, N. (2011) Children Experiencing Domestic Violence: A research review. Dartington: Research in Practice.
-
Woolgar, M. (2013) ‘The practical implications of the emerging findings in the neurobiology of maltreatment for looked after and adopted children: Recognising the diversity of outcomes’. Adoption & Fostering, 37 (3) 237-252.
-
Stanley, N. (2011) op. cit.
-
Raws, P. (2016) Understanding Adolescent Neglect: Troubled teens. A study of the link betweenparenting and adolescent neglect. London: The Children's Society.
-
For a scope of the evidence relating to adolescent risk see: Hanson, E. and Holmes, D. (2014): That Difficult Age: Developing a more effective response to risks in adolescence. Dartington: Research in Practice.
-
Rees, G., Gorin, S., Jobe, A., Stein, M. et al (2010) Safeguarding Young People: Responding to young people aged 11 to 17 who are maltreated. London: The Children's Society.
-
Hanson, E. and Holmes, D. (2014) op. cit.
-
Hicks, L. and Stein, M. (2010) Neglect Matters. A multi-agency guide for professionals working together on behalf of teenagers. London: DCSF.
-
ibid.
-
Sidebotham, P. et al (2016) op. cit.
-
Rees, G. et al (2010); Hanson, E. and Holmes, D. (2014) op. cit.
-
Biehal, N., Ellison, S. and Sinclair, I. (2012) ‘Intensive fostering: An independent evaluation of MTFC in an English setting’, Adoption & Fostering 36 (1) 13-26.
-
Stock, L., Spielhofer, T. and Gieve, M. (2016) Independent Evidence Review of Post-adoption Support Interventions. London: Department for Education
-
HM Government (2015) Working Together to Safeguard Children. A guide to inter-agency working to safeguard and promote the welfare of children.
-
Turney, D., Platt, D., Selwyn, J. and Farmer, E. (2011) Social Work Assessment of Children in Need: What do we know? Messages from research. London: Department for Education.
-
Research in Practice (2016) Impact of the Family Justice Reforms: Phase 3 – exploring variation across 21 local authorities. London: Department for Education.
-
Children looked after in England (including adoption) year ending 31 March 2016 SFR41/2016
-
Specific data on this are not provided in the datasets.
-
Department for Education (2015) The Children Act 1989 guidance and regulations Volume 2: Care planning, placement and case review
-
Schofield, G., Beek, M. and Ward, E. (2012) ‘Part of the family: Planning for permanence in long-term family foster care’. Children and Youth Services Review, 34 (1) 244-253.
Sinclair I., Baker C., Lee J. and Gibbs, I. (2007) The Pursuit of Permanence: A study of the English child care system. London: Jessica Kingsley Publishers.
Boddy, J. (2013) Understanding Permanence for Looked After Children: A review of research for the Care Inquiry. [No longer online]
-
For further information see: Court orders and pre-proceedings
-
The Children Act 1989 guidance and regulations Volume 2: Care planning, placement and case review (pp22-23)
-
Moran, L., Devaney, C., McGregor, C. and Reddy, J. (2016) Scoping Review of International and Irish Literature on Outcomes for Permanence and Stability for Children in Care. National University of Ireland.
Selwyn, J. (2010) 'The challenges in planning for permanency'. Adoption & Fostering, 34 (3), 32-37.
-
Boddy, J. (2013) op. cit. (p.4)
-
Minnis, M. and Walker, S. (2012) The Experiences of Fostering and Adoption Processes – The views of children and young people: literature review and gap analysis. NFER.
-
Department for Education (2015) The Children Act 1989 guidance and regulations Volume 2: Care planning, placement and case review.
-
Argent H (2009) ‘What's the problem with kinship care?’ Adoption & Fostering, 33 (3), 6-14.
-
7 Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship:
Experiences, challenges and outcomes. London: Department for Education. -
Adoption: A new approach (2000)
-
Department for Education (2017) Special Guardianship: Statutory guidance for local authorities (p.6)
-
For further information see: Wade, J. et al (2014) op. cit.
-
ibid.
-
Department for Education (2014) Court orders and pre-proceedings
-
Sinclair, I. and Wilson, K. (2009) 'Foster care in England'. In Schofield, G. and Simmonds, J. (eds) The
Child Placement Handbook. Research, policy and practice. London: BAAF. -
Children looked after in England (including adoption) year ending 31 March 2016 SFR41/2016
-
See section 3.143 of The Children Act 1989 guidance and regulations Volume 2: Care planning,
placement and case review -
Sinclair, I. and Wilson, K. (2009) op. cit.
-
Department for Education (2015) The Children Act 1989 guidance and regulations Volume 2: Care
planning, placement and case review -
Department for Education (2015) Guide to the Children's Homes Regulations including the quality
standards -
Narey, M. (2016) Residential Care in England (p.5)
-
Berridge, D., Biehal, N. and Henry, L. (2012) Living in Children’s Residential Homes. London:
Department for Education. -
Department for Education (July 2016) Looked after children in residential care: Analysis
-
Narey, M. (2016) op. cit.
-
ibid.
-
Children looked after in England (including adoption) year ending 31 March 2016 SFR41/2016
-
ibid.
-
ibid.
-
Harwin, J., Alrouh, B., Palmer, M., Broadhurst, K. and Swift, S. (2015) A National Study of the Usage of
Supervision Orders and Special Guardianship Orders over Time (2007-2016). Briefing paper no 1: Special
guardianship orders. Nuffield Foundation. -
Selwyn, J., Wijedesa, D. and Meakings, S. (2014) Beyond the Adoption Order: Challenges,
interventions and adoption disruption. London: Department for Education. -
Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship: Experiences, challenges and outcomes. London: Department for Education.
-
Selwyn, J. et al (2014) op. cit.
-
ibid.
-
Harwin, J. et al (2015) op. cit.
-
ibid.
-
ibid.
-
Children looked after in England (including adoption) year ending 31 March 2016: Table E1
-
Selwyn, J. et al (2014) op. cit.
-
Department for Education (2012) An Action Plan for Adoption: Tackling delay.
-
Selwyn, J. et al (2014) op. cit.
-
Looked after children and young people: NICE public health guideline 28.
-
Farmer, E. and Dance, C. (2016) ‘Family finding and matching in adoption: What helps to make a good
match?’ British Journal of Social Work, 46 (4) 974-992 -
Schofield, G., Beek, M., Ward, E. and Sellick C (2011) Care Planning for Permanence in Foster Care.
Norwich: University of East Anglia. -
Sinclair, I. (2005) Fostering Now. Messages from research. London: Jessica Kingsley Publishers. Schofield, G. et al (2011) op. cit.
-
Schofield, G. and Beek, M. (2014) The Secure Base Model: Promoting attachment in foster care and adoption. London: BAAF.
Moran, L., Devaney, C., McGregor, C. and Reddy, J. (2016) Scoping Review of International and Irish Literature on Outcomes for Permanence and Stability for Children in Care. National University of Ireland.
-
Shemmings, D. (2011) Attachment in Children and Young People. Frontline Briefing. Dartington: Research in Practice.
Howe, D. (2009) 'The impact of histories of abuse and neglect on children in placement'. In Schofield, G. and Simmonds, J. (eds) The Child Placement Handbook. Research, policy and practice. London: BAAF.
-
Brown, R and Ward, H. (2013) Decision-making within a child’s timeframe. An overview of current research evidence for family justice professionals concerning child development and the impact of maltreatment. Childhood Wellbeing Research Centre.
-
Howe, D. (2009) op. cit.
-
Looked after children and young people: NICE public health guideline 28
-
Children looked after in England (including adoption) year ending 31 March 2016 SFR41/2016. (NB: this
data does not separate out children subject to care orders and those in care under s.20 voluntary
arrangements). -
Department for Education (2013) Data Pack. Improving permanence for looked after children. London:
DfE. -
Oosterman, M. (2007) 'Disruptions in foster care: Review and meta-analysis'. Children and Youth Services Review, 29 (1) 53-76.
-
Rubin, D., O’Reilly, A., Luan, X. and Localio, A. (2007) 'The impact of placement stability on behavioural well-being for children in foster care'. Pediatrics, 119 (2) 336-344
-
Sinclair, I. and Wilson, K. (2009) ‘Foster care in England’. In Schofield, G. and Simmonds, J. (eds) The Child Placement Handbook. Research, policy and practice. London: BAAF.
-
Lord, J. and Borthwick, S. (2009) 'Planning and placement for sibling groups'. In Schofield, G. and Simmonds, J. (eds) The Child Placement handbook. Research, policy and practice. London: BAAF.
-
Saunders, H. and Selwyn, J. (2010) Adopting Large Sibling Groups. Experiences of agencies and adopters in placing sibling groups for adoption from care. University of Bristol. [No longer online]
-
Children's Rights Director for England (2014) Children’s Care Monitor 2013/14: Children on the state of social care in England. London; Office of the Children's Rights Director.
-
Saunders, H. and Selwyn, J. (2010) op. cit.
-
Lord, J. and Borthwick, S. (2009) op. cit.
-
Saunders, H. and Selwyn, J. (2010) op. cit
-
Hegar, R. (2005) 'Sibling placement in foster care and adoption: an overview of international research'.
Children and Youth Services Review, 27 (7) 717-739. -
ibid.
-
ibid.
-
Schofield, G. and Stevenson, O. (2009) ‘Contact and relationships between fostered children and their birth families’. In (eds) Schofield, G. and Simmonds, J. The Child Placement Handbook. Research, policy and practice. London: BAAF.
-
Boddy, J. (2013) Understanding Permanence for Looked After Children: A review of research for the Care Inquiry. (p.26) [No longer online]
-
Schofield, G. and Stevenson, O. (2009) op. cit.
-
Humphreys, C. and Kiraly, M. (2011) 'High-frequency family contact: A road to nowhere for infants'.
Child & Family Social Work, 16 (1) 1-125. -
Kenrick, J. (2009) 'Concurrent planning: A retrospective study of the continuities and discontinuities of care and their impact on the development of infants and young children placed for adoption by the Coram Concurrent Planning Project'. Adoption & Fostering, 33 (4) 5-18.
Schofield, G. and Simmonds, J. (2011) ‘Contact for infants subject to care proceedings’. Adoption & Fostering, 35 (4) 70-74.
-
Cafcass and ADCS (2013) ‘Good practice guidance note: Contact’. [No longer online]
-
Research in Practice (2015) Contact: Making good decisions for children in public law. What the research tells us about planning contact in assessment, fostering, adoption and kinship care. Dartington: Research in Practice.
-
Young, J. and Neil, E. (2009) ‘Contact after adoption’. In (eds) Schofield, G. and Simmonds, J. The Child Placement Handbook. Research, policy and practice. London: BAAF.
-
Adams, P. (2012) Planning for Contact in Permanent Placements. Good practice guide. London: BAAF.
-
Lord, J. and Borthwick, S. (2009) 'Planning and placement for sibling groups'. In Schofield, G. and Simmonds, J. (eds) The Child Placement handbook. Research, policy and practice. London: BAAF.
-
Neil, E., Cossar, J, Jones, C, Lorgelly P. and Young, J. (2011) Supporting Direct Contact after Adoption. London: BAAF.
-
ibid.
-
Neil, E., Beek, M. and Ward, E. (2014) Contact After Adoption: A follow up in late adolescence. University of East Anglia.
-
Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship: Experiences, challenges and outcomes. London: Department for Education.
Research in Practice (2015) Impact of the Family Justice Reforms on Front-line Practice Phase Two: Special Guardianship Orders. London: Department for Education.
-
Wade, J. et al (2014) op. cit.
-
ibid.
-
Research in Practice (2015) Contact: Making good decisions for children in public law. What the research tells us about planning contact in assessment, fostering, adoption and kinship care. Dartington: Research in Practice. (p.14)
-
For further information see: Biehal, N., Ellison, S., Baker, C. and Sinclair, I. (2010) Belonging and Permanence: Outcomes in long-term foster care and adoption. London: BAAF.
-
Wade, J., Biehal, N., Farrelly, N. and Sinclair, I. (2010) Maltreated Children in the Looked After System: A comparison of outcomes for those who go home and those who do not. London: Department for Education.
-
ibid.
-
ibid.
-
Farmer, E. and Lutman, E. (2010) Case Management and Outcomes for Neglected Children Returned to their Parents: A five year follow-up study. London: Department for Education.
-
Wilkins, M. and Farmer, E. (2015) Reunification: An evidence-informed framework for return home practice. London: NSPCC.
-
Farmer, E. and Lutman, E. (2010) op. cit.
-
Davies, C. and Ward, H. (2012) Safeguarding Children Across Services: Messages from research on identifying and responding to child maltreatment. London: Jessica Kingsley Publishers
-
Wilkins, M. and Farmer, E. (2015) op. cit.
-
ibid.
Hyde-Dryden, G., Holmes, L., Lawson, D. and Blackmore, J. (2015) Evaluation of Taking Care: A practice framework for reunification. London: NSPCC.
-
Biehal, N., Ellison, S., Baker, C. and Sinclair, I. (2010) Belonging and Permanence: Outcomes in longterm foster care and adoption. London: BAAF.
-
For a summary see: Adoption Research Initiative Summary 1: Belonging and permanence: Outcomes in
long-term foster care and adoption. -
Biehal, N. et al (2010) op.cit.
-
McSherry, D., Malet M. and Weatherall, K (2016) 'Comparing long-term placements for young children in care: Does placement type really matter?' Children and Youth Services Review, 69, 56-66.
-
Berridge, D., Biehal, N. and Henry, L. (2012) Living in Children’s Residential Homes. London: Department for Education.
-
Department for Education (2014) Children's Homes Data Pack
-
Selwyn, J., Wijedesa, D. and Meakings, S. (2014) Beyond the Adoption Order: Challenges, interventions and adoption disruption. London: Department for Education.
-
8 According to the researchers, the marked level is in the clinical range and is highly predictive of
psychiatric impairment. -
Selwyn, J. et al (2014) op. cit.
-
ibid.
-
Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship: Experiences, challenges and outcomes. London: Department for Education.
-
ibid.
-
Winokur, M., Holtan, A. and Batchelder, K. (2014) Kinship care for the safety, permanency, and wellbeing of children removed from the home for maltreatment. Cochrane Database of Systematic Reviews.
-
Selwyn, J., Wijedesa, D. and Meakings, S. (2014) Beyond the Adoption Order: Challenges, interventions and adoption disruption. London: Department for Education
-
Data for the three orders were available for different time periods: adopted group for 12 years, the special guardianship order for five years and residence order data for six years. Therefore, to ensure a ‘like with like’ comparison, survival analysis was used based on a maximum of a five year follow-up period.
-
Selwyn, J. et al (2014) op. cit.
-
ibid.
-
Wade, J. et al (2014) op. cit.
-
Selwyn, J. et al (2014) op. cit.
-
Hunt, J Waterhouse, S. and Lutman, E. (2008) Keeping them in the Family: Outcomes for children placed in kinship care through care proceedings. London: BAAF.
-
Selwyn, J. and Masson, J. (2014) 'Adoption, special guardianship and residence orders: A comparison of disruption rates'. Family Law, December.
-
Research in Practice (2016) Impact of the Family Justice Reforms: Phase 3 – exploring variation across 21 local authorities. London: Department for Education.
Research in Practice (2015) Impact of the Family Justice Reforms on Front-line Practice Phase Two: Special Guardianship Orders. London: Department for Education.
-
Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship: Experiences, challenges and outcomes. London: Department for Education.
-
Research in Practice (2015) op. cit.
-
ibid.
-
Wade, J. et al (2014) op. cit.
-
The data compares children aged 10 and over so that a meaningful comparison can be made with other
placements. -
Department for Education (2014) Children's Homes Data Pack
-
ibid.
Selwyn, J., Wijedesa, D. and Meakings, S. (2014) Beyond the Adoption Order: Challenges, interventions and adoption disruption. London: Department for Education.
Schofield, G., Beek, M., Ward, E and Sellick, C. (2011) Care Planning for Permanence in Foster Care. Norwich: University of East Anglia
-
Selwyn, J. et al (2014) op. cit.
-
Farmer, E. (2009) ‘Making kinship care work’. Adoption & Fostering, 33 (3) 15-27
-
Farmer, E. and Moyers, S. (2008) Kinship Care: Fostering effective family and friends placements. Jessica Kingsley Publishers.
-
Nandy, S., Selwyn, J,. Famer, E. and Vaisey, P. (2011) Spotlight on Kinship Care: Using Census microdata to examine the extent and nature of kinship care in the UK at the turn of the twentieth century. University of Bristol.
-
Wade, J. et al (2014) op. cit.
-
Schofield, G. et al (2011) op. cit.
-
Ottaway, H. and Selwyn, J. (2016) ‘No-one told us it was going to be like this’: Compassion fatigue and
foster carers. University of Bristol. -
Oosterman, M. (2007) 'Disruptions in foster care: review and meta-analysis'. Children and Youth Services Review, 29 (1) 53-76.
Selwyn, J. et al (2014) op.cit.
-
Quinton, D. (2012) Rethinking Matching in Adoptions from Care: A conceptual and research review. London: BAAF.
-
Wade, J. et al (2014) op.cit.
-
Biehal, N., Ellison, S., Baker, C. and Sinclair, I. (2010) Belonging and Permanence: Outcomes in longterm foster care and adoption. London: BAAF. (p.262)
-
Selwyn, J., Wijedasa, D. and Meakings, S (2014) Beyond the Adoption Order: Challenges, interventions and adoption disruption. London: Department for Education.
-
Biehal, N. et al (2010) op. cit.
-
Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship: Experiences, challenges and outcomes. London: Department for Education.
-
4 Farmer, E., Selwyn, J. and Meakings, S. (2013) '"The children say you're not normal because you don't live with your parents": Children's views of living with informal kinship carers’. Child & Family Social Work, 18 (1) 25-34.
-
Outcomes for children looked after by local authorities in England, 31 March 2015 SFR11/2016
-
Berridge, D. and Saunders, H. (2009) 'The education of fostered and adopted children'. In Schofield, G. and Simmonds, J. (eds) The Child Placement Handbook. Research, policy and practice. London: BAAF.
-
O'Higgins, A., Sebba, J. and Luke, N. (2015) What is the Relationship between being in Care and the Educational Outcomes of Children? An international systematic review. Oxford: Rees Centre.
-
8 Sebba, J., Berridge, D., Luke, N., Fletcher, J. et al (2015) The Educational Progress of Looked After Children in England: Linking care and educational data. Oxford: Rees Centre.
-
ibid.
-
ibid.
-
Selwyn, J., Wijedasa, D. and Meakings, S (2014) Beyond the Adoption Order: Challenges, interventions and adoption disruption. London: Department for Education.
Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship: Experiences, challenges and outcomes. London: Department for Education.
Biehal, N., Ellison, S., Baker, C. and Sinclair, I. (2010) Belonging and Permanence: Outcomes in long-term foster care and adoption. London: BAAF.
-
For further information see: Boddy, J. (2013) Understanding Permanence for Looked After Children: A review of research for the Care Inquiry. [No longer online]
-
Dance, C. and Farmer, E. (2014) 'Changing lives and changing minds: The experiences of adoptive parents from application to approval'. Adoption & Fostering, 38 (2) 101-114
-
For a review see: Ward, H., Brown, R. and Hyde-Dryden, G. (2014) Assessing Parental Capacity to Change when Children are on the Edge of Care: An overview of current research evidence. London: Department for Education.
-
Hunt, J. (2015) Assessing and Supporting Family and Friends Care: Practice tool. Dartington: Research in Practice.
-
A study currently being conducted by Judith Masson and colleagues will provide detailed quantitative findings on the operation of and decision-making in care proceedings under the Public Law Outline 2014 and therefore following the key decisions (see section 1.1 above) of Re B, Re B-S and Re R. The study will also provide information about long-term outcomes for children subject to care proceedings in 2010 (using DfE administrative data and the Welsh equivalents), and allow comparison of outcomes one year after the end of proceedings for these children and children subject to care proceedings in 2014-15. It includes SGOs made in the care proceedings above, including details of the assessment process and the time (if any) the child spent with the SGO carers before the order was made.
-
The University of Strathclyde is currently engaged in a project on the assessment and support of sibling relationships of long-term fostered and adopted children.
-
Working together to safeguard children. A guide to inter-agency working to safeguard and promote the
welfare of children. [No longer online] -
Flood, S. and Holmes, D. (2016) Child neglect and its relationship to other forms of harm- responding effectively to children's needs: Executive summary. Dartington: Research in Practice. (p.3)
References
Adams (2012) Planning for Contact in Permanent Placements. Good Practice Guide. London: BAAF.
Adoption and Children Act 2002. The Stationery Office.
Ainsworth, M., Biehar, M. and Waters, E. (1978) Patterns of Attachment: A psychological study of the strange situation. New Jersey: Lawrence Erlbaum Associates.
Allnock, D. 'Child Neglect. The research landscape'. In Gardner, R. (2016) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
Allnock, D. (2016) Exploring the Relationship between Neglect and Adult-perpetrated Intrafamilial Child Sexual Abuse: Evidence Scope 2. Dartington: Research in Practice.
American Psychiatric Association (2013) Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
Argent H (2009) ‘What's the problem with kinship care?’ Adoption and Fostering, 33 (3), 6-14.
Barlow, J. (2016) 'The effects of emotional neglect during the first two years of life'. In Gardner R. (2016) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
Baynes, P. and Holland, S. (2012) ‘Social work with violent men: A child protection file study in an English local authority.’ Child Abuse Review 21 (1) 53-65.
Bazalgette, L., Rahilly, T. and Trevelyan, G (2015) Achieving emotional wellbeing for looked after children. A whole system approach. London: NSPCC
Beckett, C., Dickens, J. and Bailey, S. (2016) Outcomes for children of shorter court decision-making processes: A follow-up study of the Tri-borough care proceedings pilot. Final report. Norwich: Centre for Research on Children and Families, University of East Anglia.
Beek, M. (2011) Adoption Research Initiative Summary 1: Belonging and permanence: Outcomes in long-term foster care and adoption. London: BAAF.
Bellis, M., Ashton, K., Hughes, K., Ford, K. et al (2015) Adverse Childhood Experiences and their impact on health-harming behaviours in the Welsh adult population. Public Health Wales NHS Trust.
Belsky, J. and de Haan, M. (2010) 'Annual Research Review: Parenting and children’s brain development: the end of the beginning'. Journal of Child Psychology and Psychiatry, 52 (4) 409–428.
Benoit, D. (2004) 'Infant-parent attachment: Definition, types, antecedents, measurement and outcome'. Paediatrics and Child Health, 9 (8) 541–545.
Bentley, H., O'Hagan, O., Raff, A. and Bhatti, I. (2016) How Safe are Our Children? The most comprehensive overview of child protection in the UK 2016. London: NSPCC.
Berridge, D. and Saunders, H. (2009) 'The education of fostered and adopted children'. In Schofield, G. and Simmonds, J. (2009) (Eds) The Child Placement Handbook. Research, policy and practice. London: BAAF.
Berridge, D., Biehal, N. and Henry, L. (2012) Living in Children’s Residential Homes. London: Department for Education.
Biehal, N., Ellison, S., Baker, C. and Sinclair, I. (2010) Belonging and Permanence: Outcomes in long-term foster care and adoption. London: BAAF.
Biehal, N., Ellison, S. and Sinclair, I. (2012) ‘Intensive fostering: An independent evaluation of MTFC in an English setting’. Adoption & Fostering, 36, (1) 13-26.
Boddy, J. (2013) Understanding Permanence for Looked After Children: A review of research for the Care Inquiry. The Care Inquiry.
Bolen R (2000) ‘Validity of attachment theory’. Trauma, Violence and Abuse. 1 (2) 128- 153.
Bowlby, J. (1980) The Making and Breaking of Affectional Bonds. London: Tavistock
Brandon, M., Bailey, S. and Belderson, P. (2010) Building on the Learning from Serious Case Reviews: A Two-Year Analysis of Child Protection Database Notifications 2007- 2009. London: Department for Education.
Brandon, M., Sidebotham, P., Bailey, S., Belderson, P. et al (2012) New Learning from Serious Case Reviews: A two year report for 2009-2011. London: Department for Education.
Brandon, M., Bailey, S., Belderson, P. and Larsson, B. (2013) Neglect and Serious Case Reviews. A report from the University of East Anglia commissioned by NSPCC. London: NSPCC.
Brandon, M., Glaser, D., Maguire, S., McCrory, E. et al (2014) Missed opportunities: indicators of neglect- what is ignored, why, and what can be done? London: Department for Education.
British Medical Association (2016) Alcohol and Pregnancy: Preventing and managing fetal alcohol spectrum disorders. London: BMA.
Brown, R and Ward, H. (2013) Decision-making within a Child’s Timeframe. An overview of current research evidence for family justice professionals concerning child development and the impact of maltreatment. London: Childhood Wellbeing Research Centre.
Brown, R. and Ward, H. (2016) Eight-year-olds Identified in Infancy as at Risk of Harm: Report of a prospective longitudinal study. London: Department for Education.
Butchart, A., Harvey, A., Mian, M. and Kahane, T. (2006) Preventing Child Maltreatment: A guide to taking action and generating evidence. Geneva: World Health Organization.
Bywaters, P., Brady, G., Sparks, T. and Bos, E. (2014) 'Inequalities in child welfare intervention rates: The intersection of deprivation and identity'. Child & Family Social Work, doi. 10.1111/cfs.12161. Accessed 17/11/16.
Bywaters, P., Bunting, L., Davidson, G., Hanratty, J. et al (2016) The Relationship between Poverty, Child Abuse and Neglect: An evidence review. York: Joseph Rowntree Foundation.
Cafcass and ADCS (2013) ‘Good practice guidance note: Contact’ Children Act 1989. The Stationery Office.
Children and Families Act 2014. The Stationery Office.
Children's Rights Director for England (2014) Children’s Care Monitor 2013/14: Children on the state of social care in England. London: Office of the Children's Rights Director.
Cleaver, H., Unell, I. and Aldgate, J. (2011) Children's Needs – Parenting Capacity. Child abuse: Parental mental illness, learning disability, substance misuse and domestic violence. London: The Stationery Office.
Coleman J (2014) Understanding Adolescence: Frontline briefing. Dartington: Research in Practice.
Contact a Family (2012) Forgotten Families. The impact of isolation on families with disabled children across the UK.
Dance, C. and Farmer, E. (2014) 'Changing lives and changing minds: The experiences of adoptive parents from application to approval'. Adoption & Fostering, 38 (2) 101-114.
Davies, C. and Ward, H. (2012) Safeguarding Children Across Services: Messages from research on identifying and responding to child maltreatment. London: Jessica Kingsley Publishers.
Dayton, C., Levendosky, A., Davidson, W. and Bogat, G. (2010) ‘The child as held in the mind of the mother: The influence of prenatal maternal representations on parenting behaviours.’ Infant Mental Health Journal, 31 (2) 220-241.
Department for Education (2012) An Action Plan for Adoption – Tackling delay. London: DfE.
Department for Education (2013) Data Pack. Improving permanence for looked after children. London: DfE.
Department for Education (2014) Children's Homes Data Pack. London: DfE.
Department for Education (2014) Court Orders and Pre-proceedings for local authorities. (Statutory guidance.) London: DfE.
Department for Education (2015) Special Guardianship Review: Report on findings. Government consultation response. London: Department for Education.
Department for Education (2015) The Children Act 1989 guidance and regulations. Volume 2: Care planning, placement and case review. London: DfE.
Department for Education (2015) Guide to the Children’s Homes Regulations including the quality standards. London: DfE.
Department for Education (2016) Children's Social Care Reform: A vision for change. London: DfE.
Department for Education (2016) Adoption: A vision for change. London: DfE.
Department for Education (2016) Putting Children First: Delivering our vision for excellent children’s social care. London: DfE.
Department for Education (2016) Characteristics of children in need: 2015 to 2016. SFR 52/2016.
Department for Education (2016) Children looked after in England (including adoption) year ending 31 March 2016. SFR41/2016.
Department for Education (2016) Looked After Children in Residential Care: Analysis. Ad-hoc notice. London: DfE.
Department for Education (2016) Outcomes for children looked after by local authorities in England, 31 March 2015. SFR11/2016.
Department for Education (2017) Special Guardianship Guidance. Statutory guidance for local authorities on the Special Guardianship Regulations 2005 (as amended by the Special Guardianship (Amendment) Regulations 2016). London: Department for Education.
Department of Health (2000) Adoption: A new approach. White paper. London: Department of Health, cm 5017.
Farmer, E. (2009) ‘Making kinship care work’. Adoption and Fostering, 33 (3) 15-27.
Farmer, E. and Moyers, S. (2008) Kinship Care: Fostering effective family and friends placements. Jessica Kingsley Publishers.
Farmer, E. and Lutman, E. (2010) Case Management and Outcomes for Neglected Children Returned to their Parents: A five year follow-up study. London: Department for Education.
Farmer, E., Selwyn, J. and Meakings, S.J. (2013) '"The children say you're not normal because you don't live with your parents": Children's views of living with informal kinship carers’. Child and Family Social Work, 18 (1) 25-34.
Farmer, E. and Dance, C. (2016) ‘Family finding and matching in adoption: What helps to make a good match?’ British Journal of Social Work, 46 (4) 974-992.
Featherstone, B., White, S. and Morris, K. (2016) Re-imagining Child Protection. Towards humane social work with families. Policy Press.
Flood, S. and Holmes, D. (2016) Child Neglect and its Relationship to other forms of Harm – Responding effectively to children's needs: Executive summary. Dartington: Research in Practice.
Ford, T., Vostanis, P., Meltzer, H. and Goodman, R (2007) ' Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households'. British Journal of Psychiatry, 190 (3) 19-325.
Gardner, R. (2008) Developing an Effective Response to Neglect and Emotional Harm to Children. University of East Anglia and NSPCC.
Gardner, R. (Ed) (2016) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
Hagell, A., Coleman, J. and Brooks, F. (2015) Key Data on Adolescence 2015. London: Association for Young People’s Health.
Hanson, E. (2016) Exploring the Relationship between Neglect and Sexual Exploitation: Evidence scope 1. Dartington: Research in Practice.
Hanson, E. and Holmes, D. (2014) That Difficult Age: Developing a more effective response to risks in adolescence. Dartington: Research in Practice.
Harwin, J., Alrouh, B., Palmer, M., Broadhurst, K. and Swift, S. (2015) A National Study of the Usage of Supervision Orders and Special Guardianship Orders over time (2007- 2016). Briefing paper no 1: Special guardianship orders. London: Nuffield Foundation.
Hegar, R. (2005) 'Sibling placement in foster care and adoption: An overview of international research'. Children and Youth Services Review, 27 (7) 717-739.
Hicks, L. and Stein, M. (2010) Neglect Matters. A multi-agency guide for professionals working together on behalf of teenagers. London: Department for Children Schools and Families.
Hildyard, K. and Wolfe, D. (2002) 'Child neglect: Developmental issues and outcomes'.
Child Abuse & Neglect, 26 (6-7) 679-695.
HM Government (2015) Working Together to Safeguard Children. A guide to inter- agency working to safeguard and promote the welfare of children. London: HM Government.
Horwath, J. (2016) 'Making a difference to the neglected child's lived experience'. In Gardner R. (Ed) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
Howe, D. (2009) ‘The impact of histories of abuse and neglect on children in placement’. In Schofield, G. and Simmonds, J. (Eds) The Child Placement Handbook. Research, policy and practice. London: BAAF.
Humphreys, C. and Kiraly, M. (2011) 'High-frequency family contact: a road to nowhere for infants'. Child & Family Social Work, 6 (1), 1-125.
Hunt, J. (2015) Assessing and Supporting Family and Friends Care: Practice tool. Dartington: Research in Practice.
Hunt, J Waterhouse, S. and Lutman, E. (2008) Keeping them in the Family: Outcomes for children placed in kinship care through care proceedings. London: BAAF.
Hyde-Dryden, G., Holmes, L., Lawson, D. and Blackmore, J. (2015) Evaluation of Taking Care: A practice framework for reunification. London: NSPCC.
Jaffee, S. and Christian, C. (2014) ‘The biological embedding of child abuse and neglect’. Social Policy Report, Vol 28 No 1.
Kenrick, J. (2009) ‘Concurrent planning: A retrospective study of the continuities and discontinuities of care and their impact on the development of infant and young children placed for adoption by the Coram Concurrent Planning project’. Adoption & Fostering, 33 (4) 5-18.
Lord, J. and Borthwick, S. (2009) 'Planning and placement for sibling groups'. In Schofield, G. and Simmonds, J. (Eds) The Child Placement handbook. Research, policy and practice. London: BAAF.
McAllister, J. and Lee, W. (2016) 'Child neglect and the development of communication'. In Gardner, R (2016) Tacking Child Neglect. Research, policy and evidence-based practice. London: Jessica Kingsley Publishers.
McCrory, E. and Viding, E. (2015) 'The theory of latent vulnerability: Reconceptualizing the link between childhood maltreatment and psychiatric disorder'. Development and Psychopathology, 27 (2) 493-505.
McSherry, D., Malet M. and Weatherall, K (2016) 'Comparing long-term placements for young children in care: Does placement type really matter?' Children and Youth Services Review, 69, 56–66.
Meltzer, H., Gatward, R., Corbin, T., Goodman, R. and Ford, T. (2003) The Mental Health of Young People Looked After by Local Authorities in England. London: The Stationery Office.
Miller, D. and Brown, J. (2014) 'We have the right to be safe'. Protecting disabled children from abuse. London: NSPCC.
Mills, C. (2007) Problems at Home, Problems at School. The effects of maltreatment in the home and children's functioning at school: an overview of recent research. London: NSPCC.
Ministry of Justice (2011) The Family Justice Review. Final report. London: Ministry of Justice.
Ministry of Justice (2016) Family Court Statistics Quarterly, England and Wales. January to March 2016. London: Ministry of Justice.
Minnis, M. and Walker, S. (2012) The Experiences of Fostering and Adoption Processes – The views of children and young people: Literature review and gap analysis. Slough: NFER.
Moran, L., Devaney, C., McGregor, C. and Reddy, J. (2016) Scoping Review of International and Irish Literature on Outcomes for Permanence and Stability for Children in Care. National University of Ireland.
Moretti, M. and Peled, M. (2004) 'Adolescent-parent attachment: Bonds that support healthy development'. Paediatrics and Child Health, 9 (8) 551-555.
Munro, E. (2011) The Munro Review of Child Protection: Final Report. A child centred system. London: The Stationery Office.
Munro, E.R. and Hardy, A. (date unknown) Placement Stability: A review of the literature. Loughborough University. Downloaded 23/01/17.
Murray, M. and Osborne, C. (2009) Safeguarding Disabled children: Practice guidance. London: DCSF.
Nandy, S., Selwyn, J., Famer, E. and Vaisey, P. (2011) Spotlight on Kinship Care: Using Census microdata to examine the extent and nature of kinship care in the UK at the turn of the twentieth century. University of Bristol.
Narey, M. (2016) Residential Care in England. Report of Sir Martin Narey’s independent review of children’s residential care. London: Department for Education.
National Adoption Leadership Board (2014) Impact of Court Judgements on Adoption. What the judgements do and do not say.
National Collaborating Centre for Mental Health (2015) Children's Attachment. Attachment in children and young people who are adopted from care, in care or at high risk of going into care. NICE Guideline 26. British Psychological Society.
National Institute for Health and Care Excellence (2015) Looked-after Children and Young People: Public health guideline PH28. NICE.
National Scientific Council on the Developing Child (2012) The Science of Neglect: The persistent absence of responsive care disrupts the developing brain. Working Paper 12.
Neil, E., Cossar, J., Jones, C. Lorgelly, P. and Young, J. (2011) Supporting Direct Contact After Adoption. London: BAAF.
Neil, E., Beek, M. and Ward, E. (2014) Contact After Adoption: A follow up in late adolescence. Norwich: University of East Anglia.
Norman R, Byambaa M, De R, Butchart A, Scott J. et al (2012) 'The long-term health consequences of child physical abuse, emotional abuse, and neglect: A systematic review and meta-analysis'. PLoS Med 9(11): e1001349. doi:10.1371/journal.pmed.1001349.
O'Higgins, A., Sebba, J. and Luke, N. What is the Relationship between being in Care and the Educational Outcomes of Children? An international systematic review. Oxford: Rees Centre.
Oosterman, M. (2007) 'Disruptions in foster care: review and meta-analysis'. Children and Youth Services Review, 29 (1) 53-76.
Ottaway, H. and Selwyn, J. (2016) ‘No-one told us it was going to be like this’: Compassion fatigue and foster carers. University of Bristol.
Platt, D. and Turney, D. (2012) 'Editorial: Parental engagement with services when children may be at risk'. Child and Family Social Work, 17 (2) 115-117.
Quinton, D. (2012) Rethinking Matching in Adoptions from Care. London: BAAF.
Radford, L., Corral, S., Bradley, C., Fisher, H. et al (2011) Child Abuse and Neglect in the UK Today. London: NSPCC.
Raws, P. (2016) Understanding Adolescent Neglect: Troubled teens. A study of the link between parenting and adolescent neglect. London: The Children's Society.
Re B (A child) [2013] UKSC 33
Re B-S (Children) [2013] EWCA Civ 1146 Re R (A Child) [2014] EWCA Civ 1625
Re W (A child) EWCA Civ 793
Rees, G., Gorin, S., Jobe, A., Stein, M. et al (2010) Safeguarding Young People: Responding to young people aged 11 to 17 who are maltreated. London: The Children's Society.
Rees, G., Stein, M., Hicks, L. and Gorin, S. (2011) Adolescent Neglect. Research, policy and practice. Jessica Kingsley Publishers.
Research in Practice (2015) Contact: Making good decisions for children in public law. What the research tells us about planning contact in assessment, fostering, adoption and kinship care. Dartington: Research in Practice.
Research in Practice (2015) Impact of the Family Justice Reforms on Front-line Practice Phase Two: Special Guardianship Orders. London: Department for Education.
Research in Practice (2016) Impact of the Family Justice Reforms: Phase 3 – Exploring variation across 21 local authorities. London: Department for Education.
Rubin, D., O’Reilly, A., Luan, X. and Localio, A. (2007). 'The impact of placement stability on behavioral well-being for children in foster care'. Pediatrics, 119 (2) 336-344.
Rushton, A. and Dance, C. (2003) 'Preferentially rejected children and their development in permanent family placements'. Child and Family Social Work, 8 (4) 257-267.
Saunders, H. and Selwyn, J. (2010) Adopting Large Sibling Groups. Experiences of agencies and adopters in placing sibling groups for adoption from care. University of Bristol.
Schofield, G. and Stevenson, O. (2009) ‘Contact and relationships between fostered children and their birth families’. In (Eds) Schofield, G. and Simmonds, J. The Child Placement Handbook. Research, policy and practice. London: BAAF.
Schofield, G., Beek, M., Ward, E. and Sellick, C, (2011) Care Planning for Permanence in Foster Care. Norwich: University of East Anglia.
Schofield, G. and Simmonds, J. (2011) ‘Contact for infants subject to care proceedings’. Adoption and Fostering, 35 (4) 70-74.
Schofield, G., Beek, M. and Ward, E. (2012) ‘Part of the family: Planning for permanence in long-term family foster care’. Children and Youth Services Review, 34 (1) 244-253.
Schofield, G. and Beek, M. (2006) Attachment Handbook for Foster Care and Adoption. London: BAAF.
Schofield, G. and Beek, M. (2014) The Secure Base Model: Promoting attachment in foster care and adoption. London: BAAF.
Schrader-McMillan, A., Barlow, J. and Glaser, D. (2014) Emotional Abuse and Neglect: Identifying and responding in practice with families. Frontline briefing. Dartington: Research in Practice.
Schumacher, J., Smith-Slep, A., and Heyman, R. (2001). ‘Risk factors for child neglect’. Aggression and Violent Behavior, 6 (203) 231-254.
Sebba, J., Berridge, D., Luke, N., Fletcher, J. et al (2015) The Educational Progress of Looked After Children in England: Linking care and educational data. Oxford: Rees Centre.
Selwyn, J. (2010) 'The challenges in planning for permanency'. Adoption & Fostering, 34 (3), 32-37.
Selwyn, J. and Masson, J. (2014) 'Adoption, special guardianship and residence orders: A comparison of disruption rates'. Family Law, (December).
Selwyn, J., Wijedasa, D. and Meakings, S. (2014) Beyond the Adoption Order: Challenges, interventions and adoption disruption. London: Department for Education.
Sempik, J., Ward, H. and Darker, I. (2008) 'Emotional and behavioural difficulties of children and young people at entry into care'. Clinical Child Psychology and Psychiatry, 13 (2) 221-233.
Shemmings, D. (2011) Attachment in Children and Young People. Frontline briefing. Dartington: Research in Practice.
Sidebotham, P. and Heron, J. (2006) 'Child maltreatment in the "children of the nineties": A cohort study of risk factors'. Child abuse & Neglect 30 (5) 497-522.
Sidebotham, P., Brandon, M., Bailey, S., Belderson, P. and others (2016) Pathways to Harm, Pathways to Protection: A triennial analysis of serious case reviews 2011 to 2014. London: Department for Education.
Sinclair, I. (2005) Fostering Now: Messages from research. London: Jessica Kingsley Publishers.
Sinclair I., Baker C., Lee J. and Gibbs I. (2007) The Pursuit of Permanence: A study of the English child care system. London: Jessica Kingsley Publishers.
Sinclair, I. and Wilson, K. (2009) ‘Foster care in England’. In Schofield, G. and Simmonds, J. (Eds) The Child Placement Handbook. Research, policy and practice. London: BAAF.
Sroufe, A. (2005) 'Attachment and development: A prospective, longitudinal study from birth to adulthood'. Attachment & Human Development, 7 (4) 349-367.
Stalker, K. and McArthur, K. (2012) ‘Child abuse, child protection and disabled children: A review of recent research’. Child Abuse Review, 21 (1) 24-40.
Stanley, N. (2011) Children Experiencing Domestic Violence: A research review. Dartington: Research in Practice.
Stock, L., Spielhofer, T. and Gieve, M. (2016) Independent Evidence Review of Post- adoption Support Interventions. London: Department for Education.
Tanner, K. and Turney, D. (2003) 'What do we know about child neglect? A critical review of the literature and its application to social work practice'. Child & Family Social Work, 8 (1) 25-34.
Thompson, R. and Raikes, H. (2003) 'Toward the next quarter-century: Conceptual and methodological challenges for attachment theory'. Development and Psychopathology, 15 (3) 691-718.
Turney, D., Platt, D., Selwyn, J. and Farmer, E. (2011) Social Work Assessment of Children in Need: What do we know? Messages from research. London: Department for Education.
Wade, J., Biehal, N., Farrelly, N. and Sinclair, I. (2010) Maltreated Children in the Looked After System: A comparison of outcomes for those who go home and those who do not. London: Department for Education.
Wade, J., Biehal, N., Farrelly, N. and Sinclair, I. (2011) Caring for Abused and Neglected Children: Making the right decisions for reunification or long-term care. London: Jessica Kingsley Publishers.
Wade, J., Sinclair, I., Stuttard, L. and Simmonds, J. (2014) Investigating Special Guardianship: Experiences, challenges and outcomes. London: Department for Education.
Ward, H., Brown, R. and Maskell-Graham, D. (2012) Young Children Suffering, or Likely to Suffer, Significant Harm: Experiences on entering education. London: Department for Education.
Ward, H., Brown, R. and Hyde-Dryden, G. (2014) Assessing Parental Capacity to Change when Children are on the Edge of Care: An overview of current research evidence. London: Department for Education.
Wastell, D. and White S (2012) 'Blinded by neuroscience: Social policy, the family and the infant brain'. Families, Relationships and Society, 1 (3) 397-414.
White, O., Hindley, N. and Jones, D (2015) ‘Risk factors for child maltreatment recurrence: an updated systematic review’. Medicine, Science and the Law, 55 (4) 259- 277
Wilkins, M. and Farmer, E. (2015) Reunification: An evidence-Informed Framework for Return Home Practice. London: NSPCC.
Winokur, M., Holtan, A. and Batchelder, K. (2014) Kinship care for the safety, permanency, and well-being of children removed from the home for maltreatment. Cochrane Database of Systematic Reviews.
Women's Aid (2015) Change that Lasts: Transforming responses to domestic violence and abuse. Women's Aid.
Woolgar, M. (2013) ‘The practical implications of the emerging findings in the neurobiology of maltreatment for looked after and adopted children: Recognising the diversity of outcomes’. Adoption & Fostering, 37 (3) 237-252.
Woolgar, M. and Baldock, E. (2015) 'Attachment disorders versus more common problems in looked after and adopted children: Comparing community and expert assessments'. Child and Adolescent Mental Health, 20 (1) 34-40.
Young, J. and Neil, E. (2009) ‘Contact after adoption’. In (Eds) Schofield, G. and Simmonds, J. The Child Placement Handbook. Research, policy and practice. BAAF.
Professional Standards
PQS:KSS - Creating a context for excellent practice | Developing excellent practitioners | Support effective decision-making | Developing excellent practitioners | Confident analysis and decision-making | Purposeful and effective social work | Child development | Adult mental ill health, substance misuse, domestic abuse, physical ill health and disability | Abuse and neglect of children | Child and family assessment | Analysis, decision-making, planning and review
PCF - Knowledge | Intervention and skills | Contexts and organisations